When discussing the problem of inducing allergy by rickets prophylaxis I have argumented earlier that there are many alternatives:
- abandon daily oral prophylaxis in the general population (attn risk of t1d, rickets, pneumonia)
- reduce daily oral dose with on demand therapy
- use only 1-3 single oral shots as in former East Germany
- exchange water-soluble by oily form
- use chemically modified isomeres
- co-application with “physiological” substances also in liver cod oil like Ca2+, P, vitamin A…
- co-application with “non-physiological” Cpg ODN…
- switch to parenteral application
There is even another option that I missed so far – the parental application. Supplementation of the mother might work if given ~6000 IU/die to the mother as been nicely shown in a new study.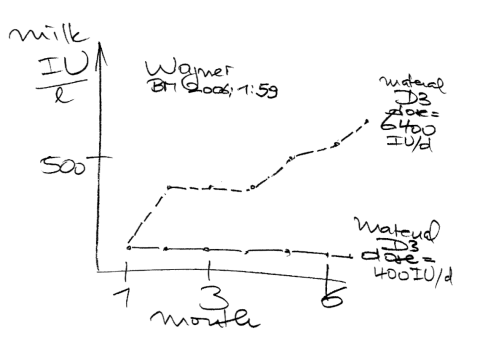
The principle is not very new – probably known since 1927. RCTs are urgently needed comparing all these treatment options while a direct oral exposure of the gut mucosa by allergen and vitamin D should be avoided.
BTW “The road not taken” is a by Robert Frost
Two roads diverged in a yellow wood,
And sorry I could not travel both
And be one traveler, long I stood
And looked down one as far as I could
To where it bent in the undergrowth.
3/9/2007
Rolf Zinkernagel made an interesting proposal last Saturday here in Munich – desenzitiation not by intradermal injection but by ultrasound directed lymphnode application.