Notice it never argues with the Society. It can’t – the RCTs are the RCTs. So it just moves the fight somewhere else. The Society shut the door on the low-normal band. This reopens it by calling that same band “deficiency.” The new “deficient” line sits exactly on the floor of the old “insufficiency” band the Society just threw out. Everyone below 50 gets relabelled. In UK Biobank, isn’t that more than half of adults?
The first pages are all rickets, seizures, osteomalacia. Sure, those are real, and I have never said otherwise. But that’s the trick – they open with mis-treated toddlers in Glasgow and close with a cutoff for sixty million people who feel fine.
They half-admit it themselves near the end: efficacy depended on VDR genotype, and “we will need to move away from using serum 25(OH)D thresholds as the only target.” Fine - so why demand a new one?
And then read who’s asking – Frontiers prints it in full:”
SC: Over the last 3 years received consultant fees from the Council for Responsible Nutrition UK CRN UK. ACT NOW Vitamin D's inception meeting was supported by CRN UK, including room hire, subsistence and travel expenses. TH: Over the last 5 years, received consultant fees from Noble Foods and an honorarium from Danone. TH's institution currently receives a sponsored PhD studentship from The Lakes Free Range Egg co. Currently instructed as an expert witness by a professional services firm in a tribunal matter concerning a nutritional supplement company. Trustee of the Nutrition Society charity. CR: Received consultancy fees during 2025 from the European Fruit Juice Association, Yoplait, General Mills, the UK Tea & Infusions Association, Tate & Lyle, Holland & Barrett, the Proprietary Association of GB, BBC Radio Scotland, the British Egg Industry Consortium, INRAE and the University of Reading. She also serves as a board member of Quality Meat Scotland, a public body. MH: Co-holder of two patents on the therapeutic use of vitamin D binding protein; honorarium and royalties as Editor-in-Chief of Feldman and Pike's Vitamin D. The remaining author(s) declared that this work was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The inception meeting paid for by the supplement trade body. Two patents on vitamin D binding protein. Royalties on a textbook.
I’m not saying the rickets isn’t real. But do you understand the urgency? I can only speculate. The ground moved – an earthquake – and an establishment defending its liturgy. Fresh scary NDNS numbers, a government that still hasn’t answered its own 2022 call for evidence, and SACN sitting at 25 as the world’s outlier.
If you are a MD: please treat vitamin D deficiency where you find it, the child kept indoors, the elderly housebound or dark skin in a Northern winter. But don’t turn half the country into patients three weeks after the biggest society on earth said stop that.
Yea, yea. Nay, nay. The rest cometh of the trade associations.
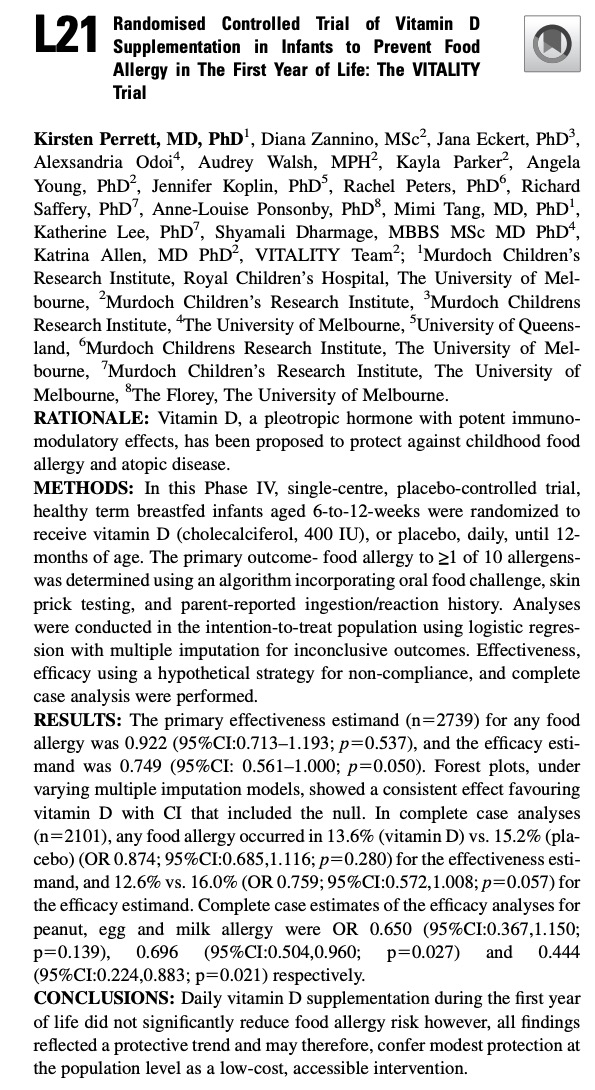
It was a long wait – 10 years – for the Vitality vitamin D study in newborns to come to an end. It is super disappointing to see now their first study abstract at the 2026 AAAAI Annual Meeting with a null result. Besides the fact that they got it wrong – Vitamin D3 supplementation was never protective but allergy risk in newborn – the following three screenshots show something that should make any methodologist uncomfortable.
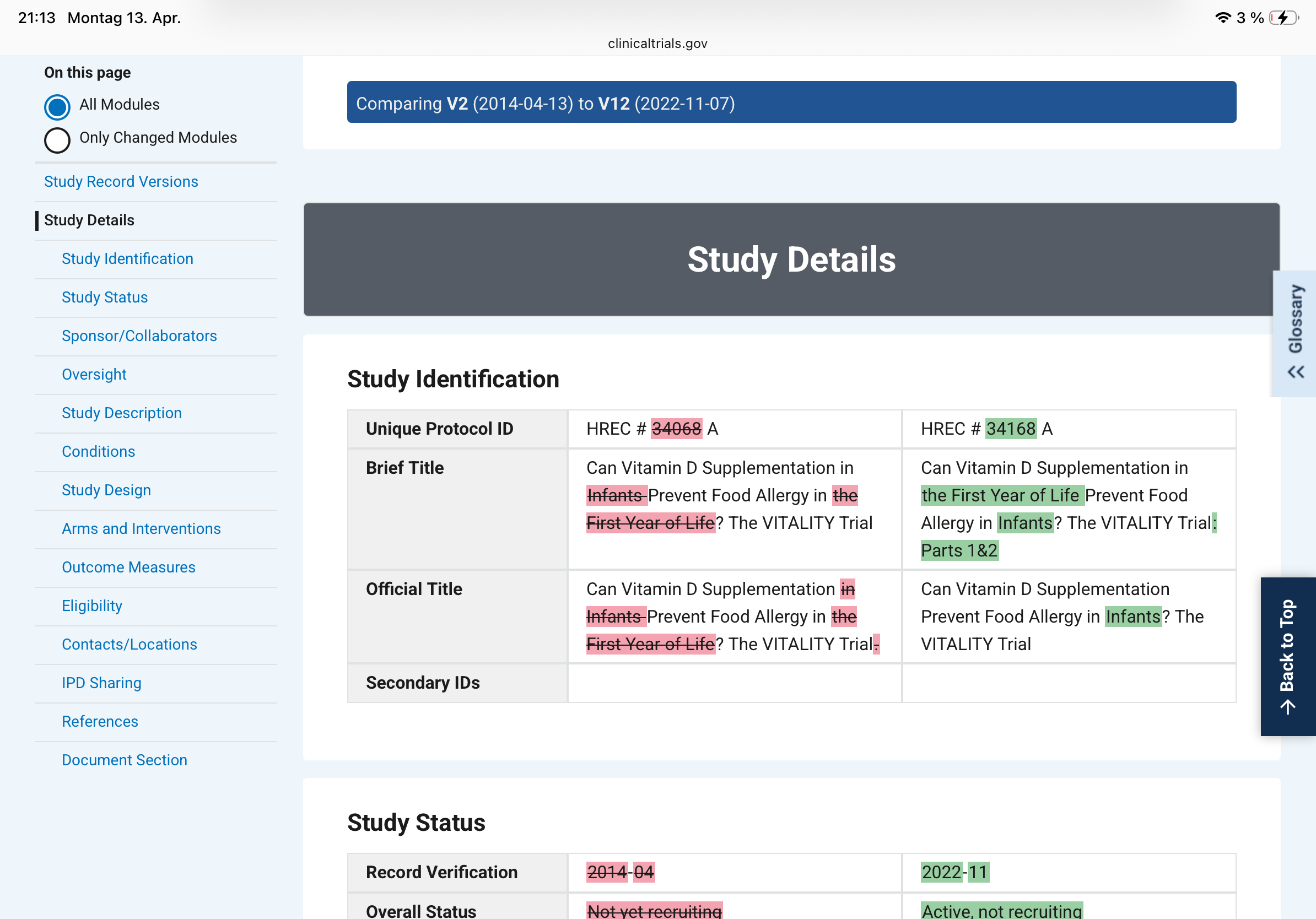
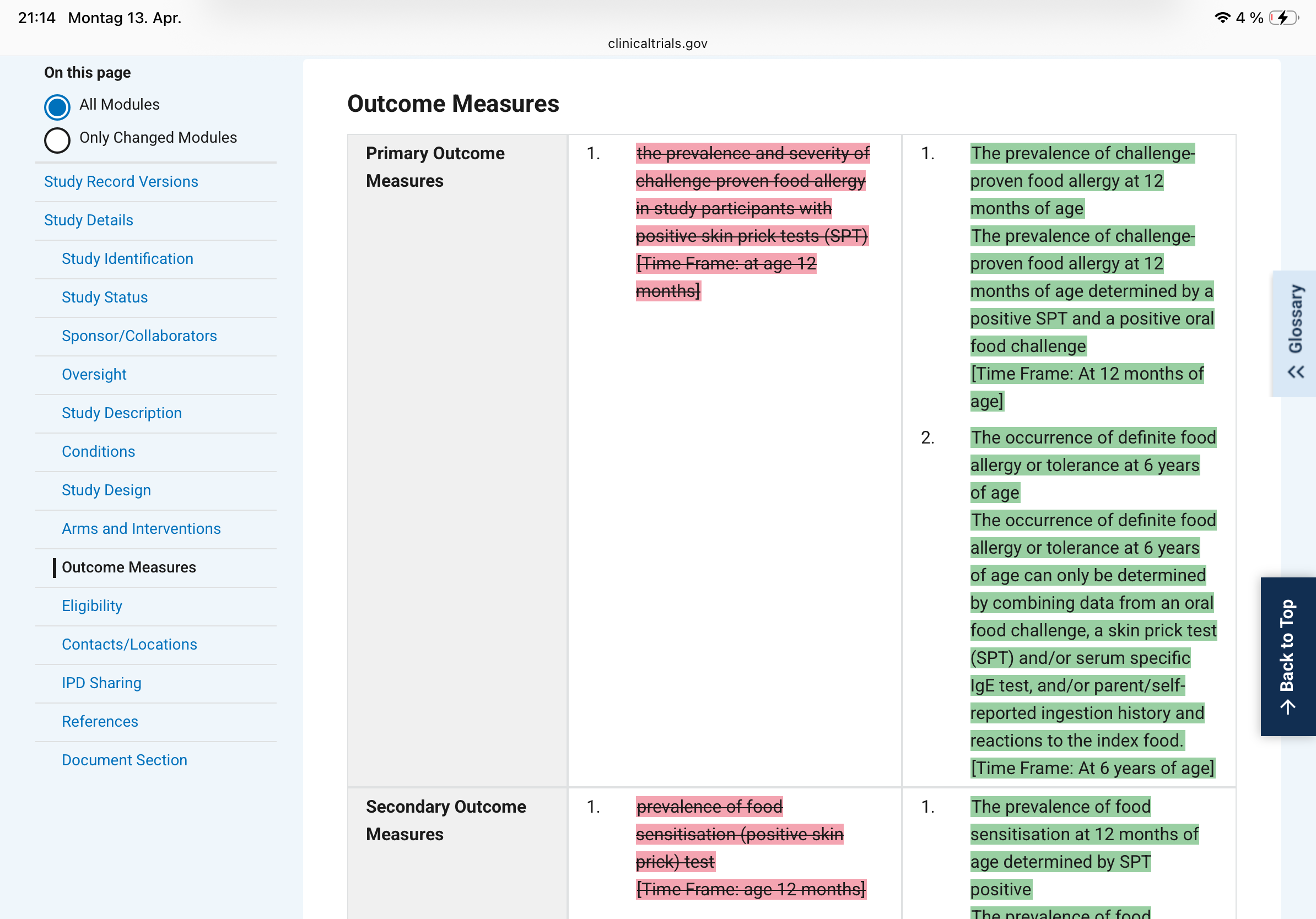
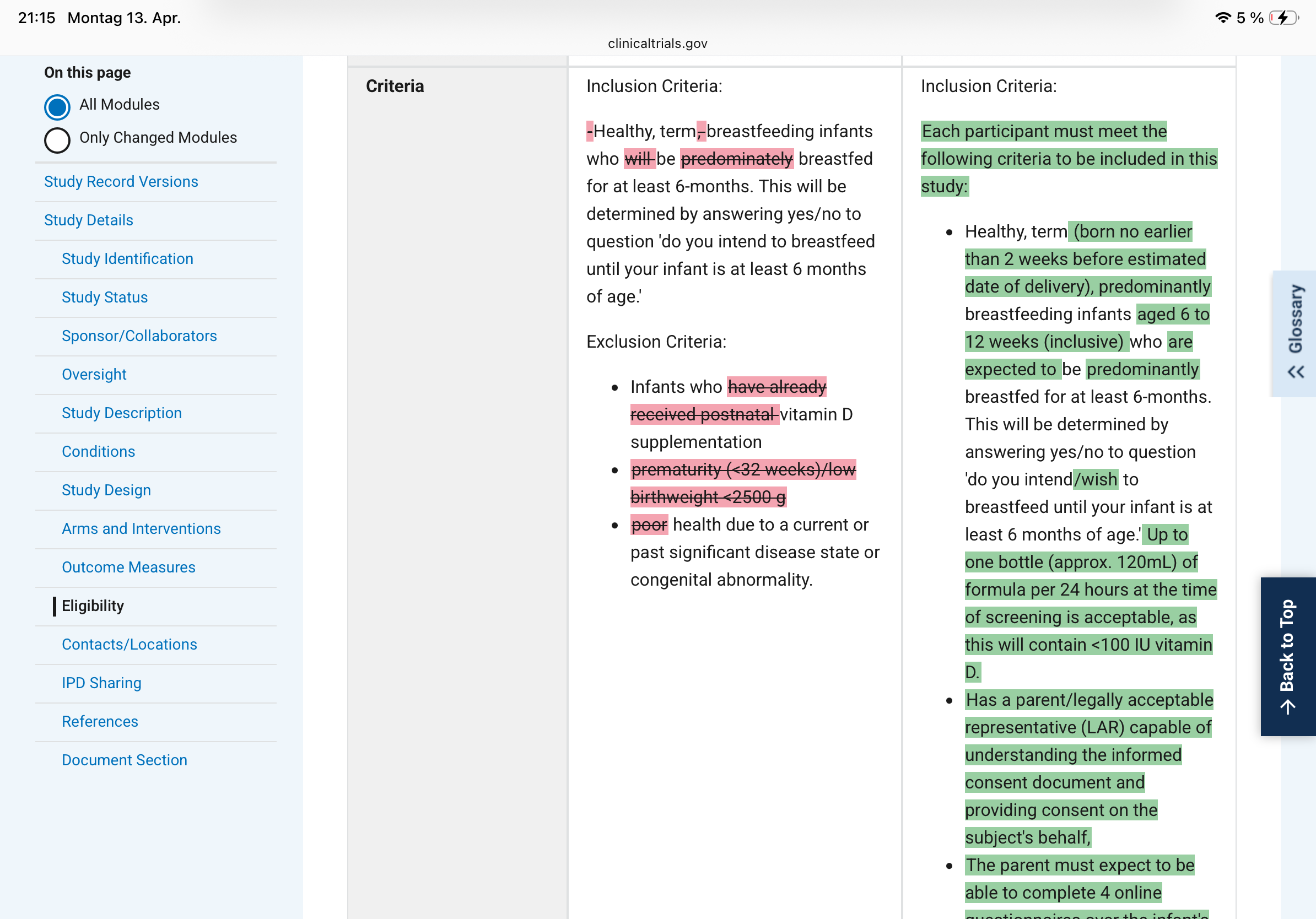
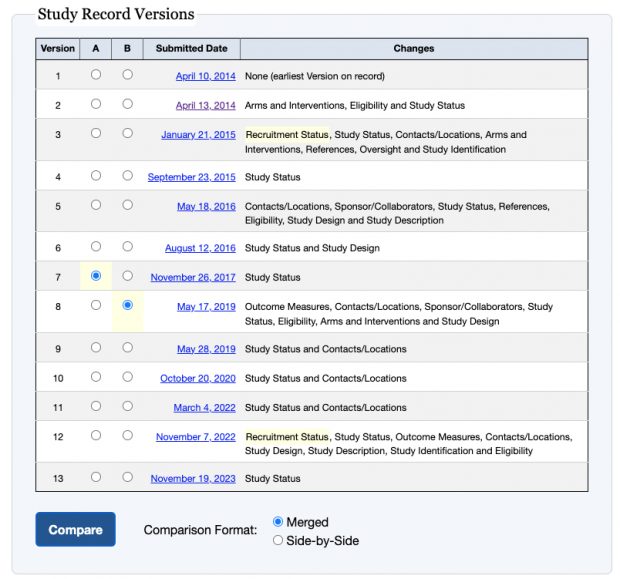
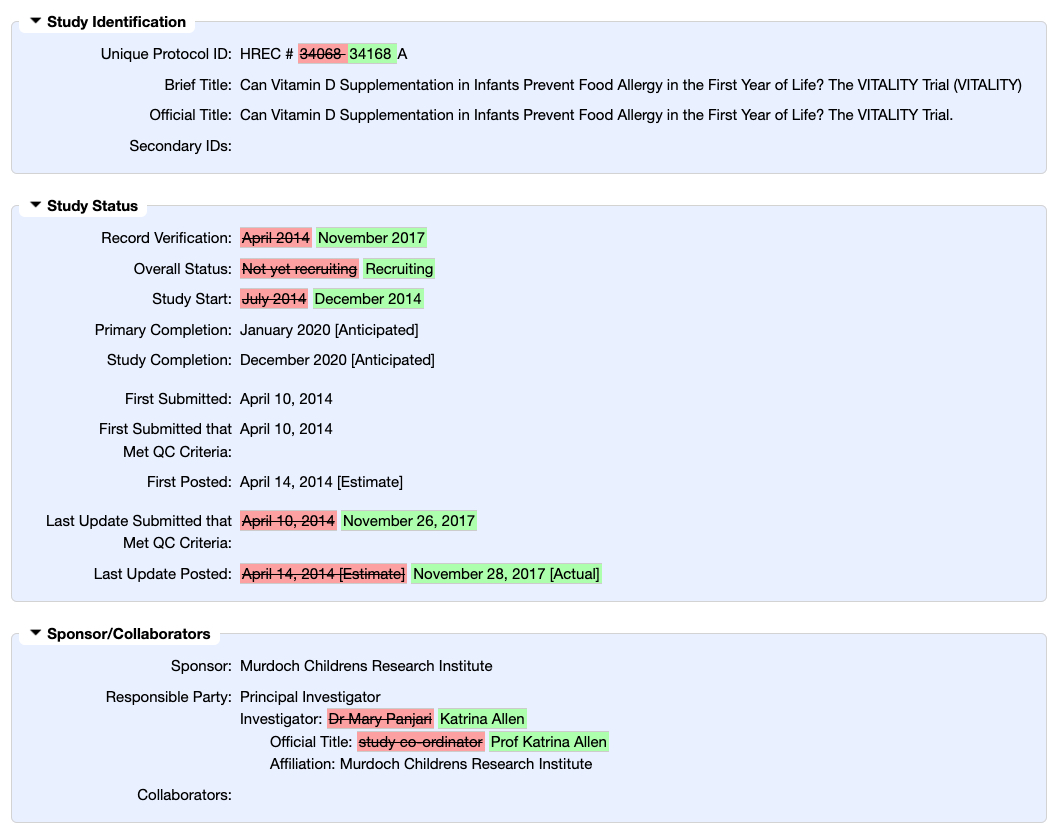
The VITALITY trial filed its first ClinicalTrials.gov record in April 2014. By November 2022 with the data at hand, version 12 shows sweeping rewrites to both the primary outcome and the inclusion criteria. Pink = deleted, green = added.
What changed, concretely:
– The original primary outcome was "prevalence and severity of challenge-proven food allergy in participants with positive skin prick tests at age 12 months." Version 12 splits this into two primaries, adds a second time point (6 years of age), and quietly drops "severity" and the SPT-positive filter. That filter was doing real work: restricting the analysis to sensitised children would have given a much smaller, higher-risk denominator.
– The inclusion criteria went from "healthy, term, breastfeeding infants" to a detailed specification with an age window (6-12 weeks), formula tolerance up to 120 mL/day, and a new informed-consent bullet. Each addition narrows or shifts the enrolled population.
Reporting two significant p-values from what are effectively subgroup analyses in an abstract whose primary result failed (p=0.537) is textbook outcome fishing. With 10 allergens tested, finding two below 0.05 by chance alone is entirely expected. In short: a failed trial has been dressed as a promising one through a combination of dual estimands, allergen subgroup mining, heavy imputation, and conclusion spin. Each element is individually defensible in isolation; together they constitute a coordinated rhetorical strategy to salvage a null result.
Why this is a fundamental problem?
Clinical trials are hypothesis tests, not explorations. The logic is identical to a one-sample t-test: you fix the null hypothesis, the test statistic, and the decision threshold before you look at the data, because the Type I error rate (your false-positive probability) is only valid under those pre-specified conditions. The moment you select or redefine your outcome after seeing interim results - even partially, even innocently - you are performing an implicit multiple comparison. You have, in effect, tested several hypotheses and reported only the one that worked.
Changing inclusion criteria mid-study is equally damaging. It redefines the population to which your result generalises. If the original enrolment targeted a broader group and the amended criteria select a more compliant or biologically distinct subgroup, the treatment effect you ultimately report belongs to a population that was never pre-specified. Reviewers and readers have no way to know whether the amendment was scientifically motivated or outcome-motivated.
The specific mischief of outcome switching
Dropping "severity" from the primary outcome is not cosmetic. A trial that fails on prevalence-plus-severity can be reframed as a success on prevalence alone. Dropping the SPT-positive filter expands the denominator, which typically dilutes an effect - unless the intervention actually works better in unselected infants, a hypothesis that was apparently not the original one. Adding a six-year follow-up endpoint transforms a 12-month study into something else entirely, with a different sample-size justification and a different regulatory profile.
What preregistration is supposed to prevent
The entire point of a trial registry is to create a timestamped public contract. Investigators declare in advance: this is our question, this is our population, this is how we will measure success. Journals and regulators can then verify that the published analysis matches the contract. When version 12 diverges this substantially from version 2, the contract has been renegotiated - and the renegotiation happened after years of data collection, when results were at least partially visible to the investigators.
This does not automatically mean misconduct. Trials genuinely need protocol amendments - safety signals emerge, recruitment proves impossible under original criteria, regulatory agencies request changes. But every such amendment requires a documented, dated rationale filed before the analysis is run, and the published paper must report both the original and amended specifications with transparent explanation. Silently absorbing eight versions of changes into a final paper, with no mention of what the original primary endpoint was, converts a confirmatory trial into a disguised exploratory one - while retaining the inferential authority of a pre-registered RCT.
The VITALITY screenshots are a clean teaching example of exactly this problem.
Sowohl das Deutsche Ärzteblatt als auch die Münchner Medizinische Wochenschrift veröffentlichten nun in kurzer Folge methodisch fragwürdige Beiträge zur Vitamin-D-Forschung. Und da sie eine enorme Reichweite in der ärztlichen Fortbildung haben, landet der Vitamin-D-Hype direkt in der Praxis mit den bekannten Folgen: Überdiagnostik, unnötige Supplementierung, wir kennen die Probleme viele Jahre zB hier. Von einer Erwiderung habe ich dennoch abgesehen, da dem Erstautor der Schlusskommentar vorbehalten bleiben sollte.
Fall 1
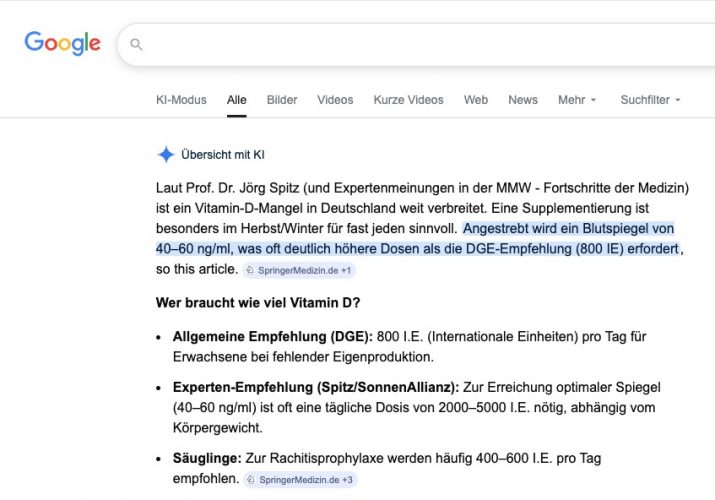
Die MMW druckt eine “Fortbildung”, genauer einen CME-Beitrag "Wer braucht wann wie viel Vitamin D?" eines lange pensionierten fachfremden Arztes (MMW Fortschr Med. 2025; 167 (S3): 76-82). Leider übernimmt die KI den Unsinn nun als Expertenmeinung…
Screenshot Google 26.3.2026
Mein Kommentar zu dem Artikel war
1. Interessenkonflikt
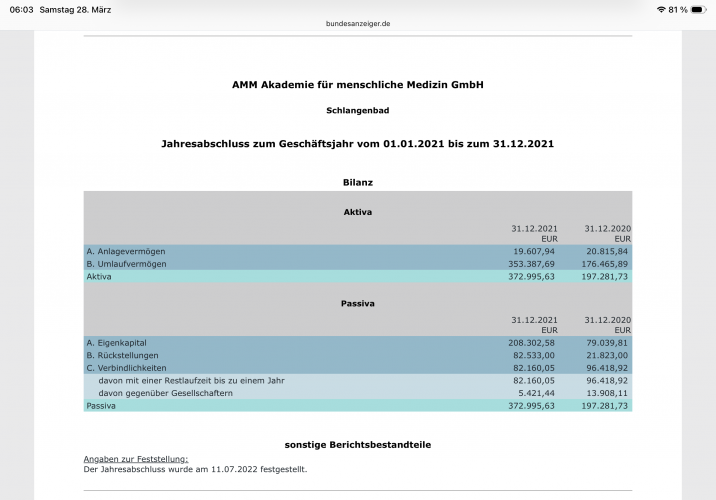
Der Autor gibt "keine Interessenkonflikte" an, betreibt jedoch die Akademie für menschliche Medizin GmbH, die kommerziell Vitamin-D-bezogene Präventionsangebote vertreibt. Diese Verbindung ist gemäß DFG- und ICMJE-Regeln deklarationspflichtig. Medwatch schreibt von 225.000€ Umsatz im Jahr 2019.
2. Epidemiologische Angaben
Die Behauptung, "90 % der Bevölkerung" hätten < 30 ng/ml Vitamin D, stützt sich auf veraltete RKI-Daten (2007-2011). Neuere Erhebungen (DEGS II, 2019) zeigen nur 30-40 % unter 50 nmol/l. → Übertriebene Darstellung eines Mangels.
3. Dosierungsempfehlung
Empfohlene 4 000-6 000 IE/Tag überschreiten den international anerkannten Upper Level von 4 000 IE/Tag (EFSA 2023). Für gesunde Erwachsene fehlt jede Evidenz.
4. Toxizität und "Coimbra-Protokoll"
Die Aussage, Werte bis 150 ng/ml seien unbedenklich, widerspricht Daten zu Hyperkalzämie und Nephrokalzinose. Das "Coimbra-Protokoll" (≥ 100 000 IE/Tag) ist nicht evidenzbasiert und medizinisch riskant.
5. Extra-skelettale Effekte
Im Artikel werden präventive Wirkungen (Demenz, KHK, Krebs, Blutdruck, Diabetes u. a.) behauptet, obwohl große RCTs (VITAL, D2d, ViDA) keinen Nutzen zeigten. Die Darstellung ist selektiv und irreführend.
6. Schwangerschaft
Die genannte 60 %ige Reduktion von Frühgeburten entstammt keiner belastbaren Quelle; die zitierte Pilotstudie (Wagner et al. 2006) weist diese Endpunkte nicht auf.
7. COVID-19-Bezug
Die angeblich 16-fache Mortalitätssteigerung bei Vitamin-D-Mangel beruht auf einem Meinungsartikel, nicht auf einer Originalstudie. Die Darstellung ist faktisch falsch.
8. Fehlende Neutralität im CME-Kontext
Der Beitrag enthält werblich anmutende Aussagen, selektive Quellenwahl (u. a. Masterarbeit Göthel 2020) und unkritische Übernahme von Hypothesen. Damit ist die formale Neutralitätsanforderung der CME-Zertifizierung (§ 4 CME-Richtlinie BÄK) nicht erfüllt.
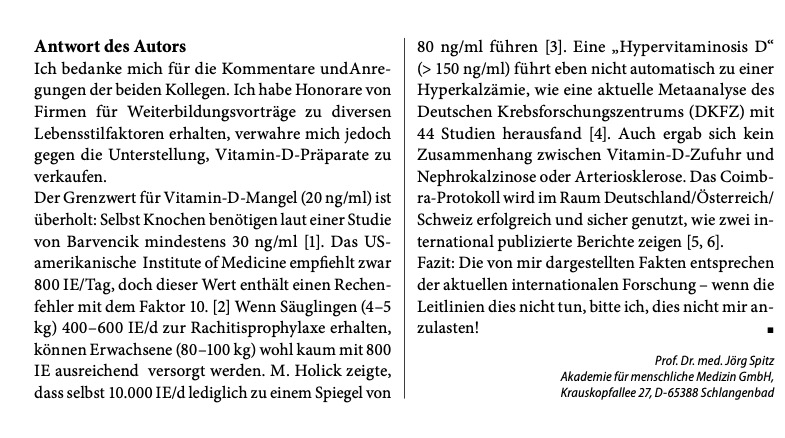
Der Chefredakteur Cornelius Heyer nimmt auf meine Reklamation zwar die CME Akkreditierung heraus, aber statt einer Korrektur oder Löschung des Beitrages, druckt die MMW einen Leserbrief nach dem Spitz das letzte Wort in der Diskussion hat. Spitz in Bhakdi Manier “Die von mir dargestellten Fakten entsprechen der aktuellen internationalen Forschung – wenn die Leitlinien das nicht tun bitte ich, dies mir nicht anzulasten”.
Screenshot 26.3.2026 Nota bene – Spitz hat nie wissenschaftlich zu dem Thema gearbeitetPassiva der Akademie für menschliche Medizin 2021
Ein beliebiger Leser der Tageszeitung ist damit nun also besser informiert als ein/e Arzt/Ärztin der die MMW abonniert hat.
Fall 2
Das Deutsche Ärzteblatt druckt die Besprechung eines Kongressabstracts “Personalisierte Vitamin D Supplementierung kann das Re-Infarktrisiko halbieren”. Wer nec ist weiss ich nicht, allerdings weiss ich genau, dass es wieder ein Märchen ist das nec hier erzählt. Der Leiter der Medizinisch-Wissenschaftlichen Redaktion des DÄ Christopher Baethge verweist mich an die journalistische Redaktion in Berlin Michael Schmedt, der allerdings auch nach Wochen immer noch nicht geantwortet hat.
New Orleans - Eine Supplementierung mit Vitamin D in individuell titrierter Dosierung kann das Risiko für einen erneuten Herzinfarkt bei vorerkrankten Personen um mehr als die Hälfte reduzieren. Das berichteten Forschende bei den Scientific Sessions 2025 der American Heart Association in New Orleans (Abstract Nr. 4382525).
[...]
Warum ist das so?
Die TARGET-D-Studie wird als Korrektur früherer negativer Vitamin-D-Studien präsentiert, mit der Behauptung, diese seien gescheitert, weil sie Vitamin D nicht "zielgerichtet" titriert hätten. Bei genauer Betrachtung reproduziert TARGET-D jedoch genau jene strukturellen Schwächen, die die Vitamin-D-Outcome-Literatur seit Jahren geplagt haben.
Der entscheidende Befund ist eindeutig: Der vordefinierte primäre Endpunkt, schwere kardiovaskuläre Ereignisse (MACE), wurde in der Intention-to-treat-Analyse nicht signifikant reduziert. Nach elementaren CONSORT-Prinzipien müsste dieses Ergebnis die Interpretation bestimmen. Stattdessen verlagert die Studie den Fokus sofort auf ein einzelnes positives Signal in einer Unterkomponente des kombinierten Endpunkts, den Folge-Myokardinfarkt. Diese Verschiebung rettet die Studie nicht, sondern verschleiert ihr negatives Hauptergebnis. Wenn ein kombinierter Endpunkt scheitert, stellt die selektive Hervorhebung einer einzelnen Komponente keine Evidenz dar, sondern narrative Verzerrung.
Die anschließende Betonung von Per-Protocol-Analysen untergräbt die Aussagekraft weiter. Diese Analysen vergleichen nicht mehr randomisierte Gruppen, sondern Untergruppen, die nachträglich anhand des Erreichens eines willkürlich gewählten Vitamin-D-Schwellenwertes definiert werden. Damit wird nicht mehr die Wirkung einer Intervention geprüft, sondern der Gesundheitszustand einer selektierten, therapietreuen, Responder Population dem einer Restgruppe gegenübergestellt, die überproportional Nicht-Responder, Gebrechliche und Patienten mit höherer Krankheitslast enthält. Der Vitamin-D-Spiegel fungiert hier als Marker guter Gesundheit und Compliance, nicht als kausaler Faktor. Genau dieser Denkfehler hat frühere Beobachtungsstudien diskreditiert, was auch in allen Umbrella Reviews klar herauskam, aber hier innerhalb eines randomisierten Designs erneut eingeführt wird.
Das Ausmaß der postrandomisierenden Selektion macht dieses Problem unübersehbar. Ein erheblicher Teil der dem Vitamin-D-Arm zugewiesenen Patienten wird aus der Per-Protocol-Analyse ausgeschlossen, weil der Zielwert nie erreicht wurde oder nur unvollständige Nachbeobachtung vorlag. Die Konditionierung auf einen postrandomisierten Biomarker zerstört die durch Randomisierung erreichte Vergleichbarkeit der Gruppen. Die daraus resultierenden Effekte sind selektionsgetrieben und nicht kausal interpretierbar.
Auch die biologische Grundannahme der Studie ist schwach fundiert. Der gewählte Zielwert von über 40 ng/ml für 25-Hydroxyvitamin D ist nicht leitlinienbasiert, entspricht nicht der neuesten Literaturund impliziert einen Schwellen- oder Dosis-Wirkungs-Effekt, der in großen randomisierten Studien und genetischen Analysen nicht bestätigt wurde. Indem der Studienerfolg über das Erreichen dieses Zielwerts definiert wird, wird der behauptete Nutzen nicht getestet, sondern implizit vorausgesetzt.
Die Darstellung der Ergebnisse verstärkt diesen Eindruck. Formulierungen wie "klinisch relevante Risikoreduktionen" oder "Reduktion des Myokardinfarktrisikos um mehr als die Hälfte" suggerieren einen kausalen Effekt, den das Studiendesign und die Resultate nicht tragen. Andere Komponenten des kombinierten Endpunkts zeigen keine konsistente Verbesserung, werden jedoch deutlich weniger betont. Der Gesamteindruck ist nicht der einer neutralen Prüfung einer Hypothese, sondern der Versuch, aus einer im Kern negativen Studie ein positives Narrativ zu extrahieren.
Insgesamt liefert TARGET-D keinen belastbaren Beleg dafür, dass eine Vitamin-D-Normalisierung das kardiovaskuläre Risiko nach akutem Koronarsyndrom senkt. Der primäre Endpunkt ist negativ, die sekundären Aussagen beruhen auf selektiver Gewichtung, und die Per-Protocol-Analysen ersetzen Randomisierung durch Adhärenz- und Selektionsmechanismen. Die Studie bestätigt letztlich nur, was die Literatur seit Langem zeigt: Niedrige Vitamin-D-Spiegel korrelieren mit schlechter Gesundheit, ihre Korrektur verändert jedoch harte kardiovaskuläre Endpunkte nicht zuverlässig. Neu an TARGET-D ist nicht die Überwindung dieser Limitationen, sondern ihre methodisch aufwendigere und potenziell irreführende Verpackung.
Die Assistentin der Chefredaktion Monia Jacobs entgegnet sinngemäß dann am 15.4. per Email, die Studie sei auf dem renommierten AHA-Kongress vorgestellt und von der AHA selbst per Pressemitteilung kommuniziert worden – ergo sei das nicht Problem des Ärzteblattes sondern der Kongressveranstalter. Der eigene Beitrag würde die Ergebnisse transparent darstellen, einschließlich des verfehlten primären Endpunkts – klassische narrative Verzerrung. Journalistische Sorgfaltspflicht verlangt, auch die gegenteilige Meinung zu benennen – sofern man denn überhaupt verstanden hat worum es hier geht.
I can’t even remember how many vitamin D studies we did, explaining how this prohormone has been discovered and how stupid guidelines came on to the scene.
And it didn't happen quietly. It wasn't a minor tweak, a footnote, or an incremental update. It was a full reversal of a doctrine that has dominated labs, clinics, public-health brochures, and countless biomarker panels for decades. A classical paper even claimed that 50% of the world population is vitamin D insufficient. For years, we had to live with the tidy triplet:
That middle category "insufficiency" became a diagnosis in itself. It justified mass screening. It justified supplementation campaigns. It justified entire clinical cultures built around chasing numbers. And then 2024 arrived.
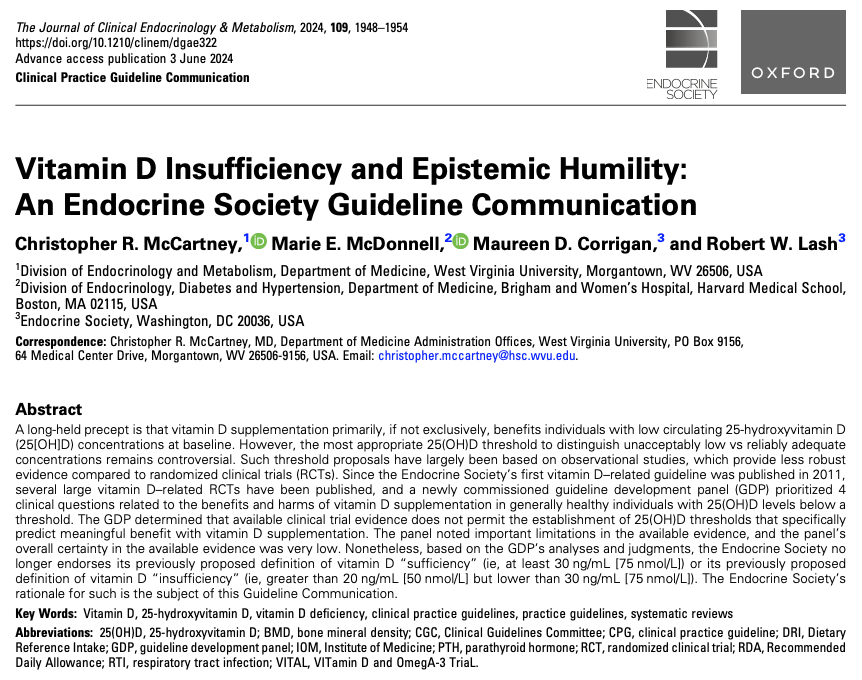
Because after reviewing all high-quality randomized trials, the Endocrine Society concluded something truly astonishing:
there is no reliable evidence that people with 25(OH)D levels between 20 and 30 ng/mL derive any clinically meaningful benefit from raising those levels
In fact, the guideline panel found that even below 20-24 ng/mL, evidence for clear benefit is surprisingly weak or uncertain - except perhaps in the very elderly, and even there the benefit didn't map neatly to a threshold. Vitamin D physiology makes the whole "insufficiency" concept biologically dubious, because serum 25(OH)D is only an external storage marker of an intracellular prohormone system - a tank that appears "empty" only in true deficiency like rickets. Let me put that differently: The category of "vitamin D insufficiency," introduced in 2011 and used worldwide, is now considered *scientifically unsupported*. The Society explicitly withdraws it.
That is not merely unusual. In the world of clinical guidelines, this is as close as you get to a scientific earthquake. Why did they withdraw it? Because the evidence never really showed what everyone assumed.
The new communication explains the problem with striking clarity:
1. Observational associations misled us.
Many early threshold claims came from correlations - low vitamin D and higher PTH, low vitamin D and lower bone density, etc. But none of this proved causality, and much of it turned out to be non-informative once RCTs were performed.
2. Surrogate markers were overinterpreted.
Calcium absorption, PTH suppression, even bone mineral density - these are *indirect* signals. They don't automatically translate into fewer fractures, fewer falls, fewer infections, or longer life. And when RCTs finally tested real outcomes, the expected clinical benefits simply weren't there.
3. Large RCTs showed no special benefit in "low-normal" ranges.
VITAL - one of the biggest vitamin D trials ever - found no difference in fractures even in participants below 24 ng/mL, and even those below 12 ng/mL did not exhibit the dramatic benefit everyone predicted (though the subgroup was very small).
4. Across thousands of participants aged 50-74, supplementation beyond the RDA made essentially no difference - including in those below the supposed thresholds.
The forest plots in the guideline communication make this visually obvious: the <20-24 ng/mL subgroups almost never differ from the overall population in any meaningful direction. (See page 5 of the document: identical risk-change estimates for falls, fractures, cancer, CVD, etc.)
We rarely see a major medical society openly dismantle one of its own most influential guidelines - not because of scandal, not because of politics, but because the evidence finally matured and said: we were wrong. And they didn't hedge. They didn't massage the language. They called the new stance what it is: epistemic humility.
Jörg Spitz ist wohl nicht der geeignete Experte für dieses Thema – es sei denn, als würde man auch Wolfgang Wodarg, Michael Meyen, Sucharit Bhakdi oder Stefan Homburg zu COVID befragen wollen.
Der Autor erklärt, dass er sich bei der Erstellung des Beitrags von keinen wirtschaftlichen Interessen leiten ließ. Er legt folgende potenzielle Interessenkonflikte offen: keine.
Der Verlag erklärt, dass die inhaltliche Qualität des Beitrags durch zwei unabhängige Gutachten bestätigt wurde. Werbung in dieser Zeitschriftenausgabe hat keinen Bezug zur CME-Fortbildung. Der Verlag garantiert, dass die CME-Fortbildung sowie die CME-Fragen frei sind von werblichen Aussagen und keinerlei Produktempfehlungen enthalten.
Gleichzeitig vertreibt Spitz aber sein “digitales Event Paket” online zur umstrittenen Hochdosis Vitamin D Therapie für 149€.
Ich hätte das nicht vermutet, aber Vitamin scheint doch ein lukratives Geschäftsmodell zu sein auch wenn man mit der Substanz selbst nichts verdienen kann. So hat medwatch schon vor längerer Zeit festgestellt
Hinter der Seite steckt der Nuklearmediziner, Buchautor und selbsternannte Präventionsexperte Jörg Spitz. Und: Vitamin D scheint eines seiner Lieblingsthemen zu sein, so hat er bereits fünf Ratgeber zu dem Vitamin veröffentlicht. Zudem betreibt er ein ganzes Netzwerk aus verschiedenen Internetseiten, die sich allesamt um Vitamin D und weitere Nahrungsergänzungsmittel drehen, etwa die Akademie für menschlichen Medizin (AMM). Die GmbH machte in 2019 einen Umsatz von 225.000 Euro - Spitz ist ihr alleiniger Mitarbeiter.
Und die Referenten der spitzen-praevention.com ? Ein echtes Panoptikum , die meisten ohne wissenschaftliche Qualifikation, dafür aber mit Missionseifer.
Yep there was some hype about 100 years ago, soon after the discovery of vitamin D by Windaus – where vitamin D / cod liver oil was used to treat tuberculosis.
Also vitamin A (also contained in high doses in cod liver oil) was used in the pre-antibiotic era as anti-infective therapy while it has lost its role being used only as some supportive add-on after during measles infection. Reliable prevention of measles by vaccination should not be confused with uncertain supportive therapy.
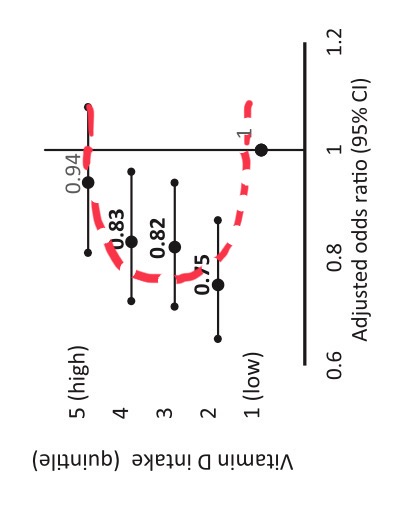
But what about vitamin D supplementation and cancer? A new study in the Annals last week show
7% reduction in cancer mortality was observed after a median cumulative follow-up of 22.3 years (1817 vs. 1943 deaths; hazard ratio [HR], 0.93 [95% CI, 0.87 to 0.99]), along with a 6% increase in CVD mortality (2621 vs. 2420 deaths; HR, 1.06 [CI, 1.01 to 1.12]).
As both risks are of borderline significance and we don’t trust P values alone, my conclusion is: vitamin D supplementation doesn’t prevent cancer.
We know it for ages (1985) that 1,25-Dihydroxyvitamin D3 suppresses human T helper cells by blocking interleukin 2 (IL 2) production. The immune effects were our main argument 2001 against oral vitamin D supplementation of newborns as it may induce later allergy . It is now funny to find now a clinical trial that tests low-dose interleukin-2 in birch pollen allergy.
I tried to update today an earlier blog post but neither VIDI (started in 2012) nor VITALITY (started in 2014) posted or published any allergy result so far.
https://classic.clinicaltrials.gov/ct2/history/NCT02112734?B=7&A=8&C=merged#StudyPageTopIf the recruitment phase lasted 2-3 years, the observation phase 1 year, results could have been published within 4 years. Instead the study is prolonged now until December 2028(!) while adding 26(!) secondary outcome measures. Two emails to previous and current PI about that remain unaswered.
Jan 9, 2024 update
According to an email yesterday, Vitality will publish primary outcome data in Q3 2024.
While our focus on allergy development was on vitamin D supplementation of newborns, the interest of Weiss et al. was on vitamin D deficiency in pregnancy. Vitamin D deficiency may not be attributed to the rise of the asthma and allergy epidemic although this remains the never ending obsession of Weiss et al.
Nevertheless, also a wrong hypothesis may lead to new insights. IKZF3 clearly is a key player where more recently heterozygous missense/LOF variants have been found in families with B-lymphopenia and EBV-associated lymphoma while the allergy proning effect is more in the 5-prime region.
The new study shows (again) that cholecalciferol suppresses the activation of the IL-2 pathway. But what is the net effect of artifical cholecalciferol exposure on naive T cells? Unfortunately the new paper narrowly focuses on cytokine production in Th2 cells only and even misses the famous Cantorna review that clearly says
Since 1983 it has been described that 1,25(OH)2D inhibited T cell proliferation and the secretion of select cytokines after mitogen stimulation. Moreover, 1,25(OH)2D directly inhibited IL-2 and IFN-γ transcription [17,18]. More recently 1,25(OH)2D has also been shown to inhibit IL-17 secretion by Th17 cells. The effects of 1,25(OH)2D on Th2 cells is more controversial with evidence that 1,25(OH)2D inhibits IL-4 transcriptionally as well as evidence that 1,25(OH)2D upregulates IL-4 in mouse and human T cells.
So we need to rephrase the finding of an “immune protective effect of vitamin D in allergic lung inflammation” to an overall “immune suppressive effect of vitamin D” which is basic textbook knowledge. Unfortunately the early origin of allergy induction remains a mystery.
Cheung and colleagues reports a survey conducted in 15 countries exploring the health and nutrition claims made in the marketing of infant formula products. The authors performed a systematic search of websites, examined packaging of formula products, and documented claims made about the formula product and citations of scientific evidence supporting those claims…
Health professionals and families lack the time to properly scrutinise claims. Industry is unlikely to change its practice given shareholder interests. Self-regulation has not worked, and responsible, ethical marketing by the formula industry seems unlikely.
The article “Vitamin D supplementation during pregnancy inhibits the activation of fetal membrane NF-κB pathway, by N. Gurkan, published in Eur Rev Med Pharmacol Sci 2022; 26 (16): 5926-5931-10.26355/eurrev_202208_29532-PMID: 36066168” has been retracted by the author as she stated that Vitamin D was used in the study as supplement and not a drug without the permission of the Ministry. Although Vitamin D is a commonly used supplement during pregnancy, the Local Ethics Committee accepted it as a drug and asked for it to be approved by the Ministry of Health. Therefore, the manuscript has been withdrawn. The Publisher apologizes for any inconvenience this may cause. https://www.europeanreview.org/article/29532
In contrast to most other endocrinologists I think that the decision is correct. Vitamin D is been chemically synthesized prohormone, underlies quality control, has benefits and side effects, could be even toxic, so it should be treated as a drug. Cudos to the Local Ethics Committee.
It seems that I missed an interesting 2017 paper that looked for disease-associated SNPs in canonical DR3 motifs. Only 7 out of 211 traits showed significant hits, one of these was self-reported allergy. When annotating these SNPs, there are only two genes: LINC00299 and TLR1
So are TLR1 & LINC00299 variant carriers more susceptible to vitamin D induced allergy?
LINC00299 (Long Intergenic Non-Protein Coding RNA 299) is a RNA Gene of largely unknown function, associated so far with allergy only on a genetic level in Framingham, href=”https://pubmed.ncbi.nlm.nih.gov/23817569/”>23andme and other studies. We don’t know so much here, the function of the long non coding RNAs
depends on subcellular localization. Depending on their niche, they specifically interact with DNA, RNA, and proteins and modify chromatin function, regulate transcription at various stages, forms nuclear condensation bodies and nucleolar organization. lncRNAs may also change the stability and translation of cytoplasmic mRNAs and hamper signaling pathways. Thus, lncRNAs affect the physio-pathological states and lead to the development of various disorders, immune responses, and cancer.
The TLR1 genetic association is found by many genetic studies, while the clinical association is probably more by an infectious origin. TLR1 is a pattern recognition receptor with a specificity for gram-positive bacteria and also included in my forthcoming exome paper as a protective factor for asthma/allergy. And we are also close to my earlier review of vitamin D, the microbiome and allergy…
Does any co-infection response during first vitamin D exposure influence allergic sensitisation? There are indeed some hints of an short-lived effect of lung group 2 innate lymphoid cells (ILC2s)
Laboratory mice cohoused for 2 weeks had impaired ILC2 responses and reduced lung eosinophilia to intranasal allergens, whereas these responses were restored in mice cohoused for ≥2 months. … These findings suggest that ILC2s respond dynamically to environmental cues and that microbial exposures do not control long-term desensitization of innate type 2 responses to allergens.
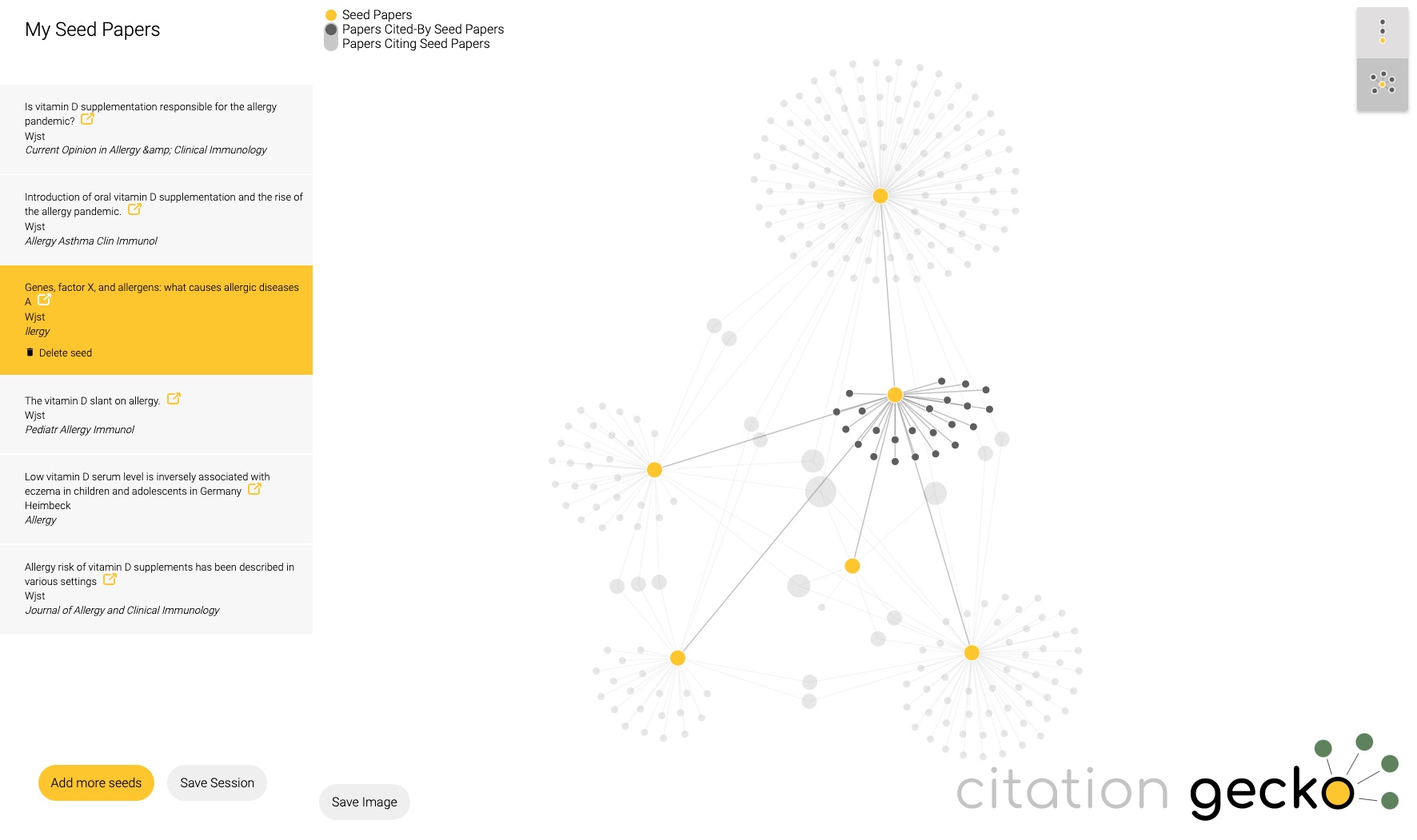
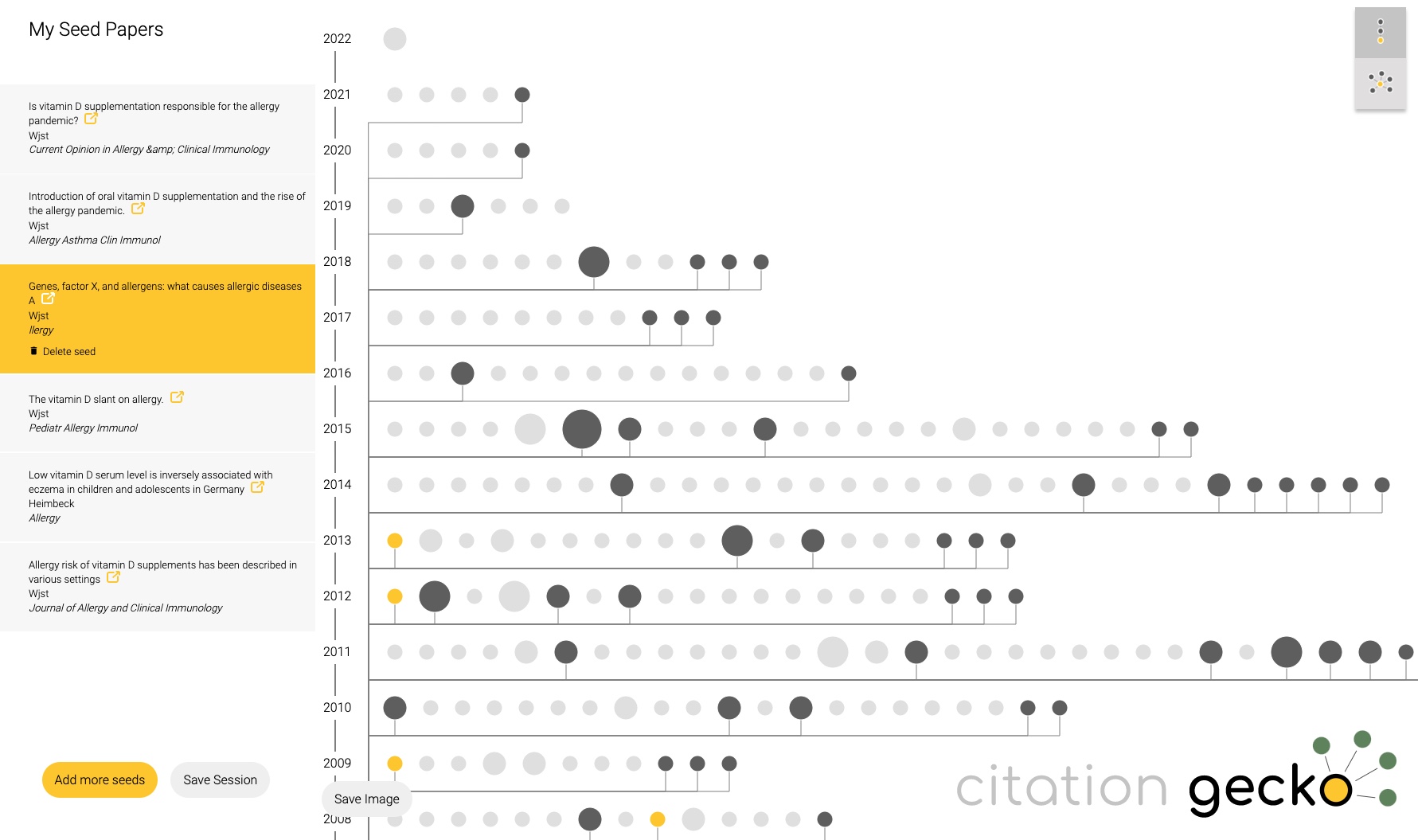
Just tried citationgecko.com on a topic that I have been working on for 2 decades. It will find rather quickly the source paper, much faster than reading through all of it. Unfortunately reviews are rated to be more influential than original data as Citation Gecko picks articles with many references.