The Gangelt study that surfaced this morning is interesting as it includes now some sound statistics using GEE models to account for household clustering (in a previous interview the lead author denied the value of statistical models). The PDF is only available an internal university server without any doi number and timestamp – not even a “preprint” at all.
Maybe I am a bit disappointed as it remains basically a cross-sectional analysis, without any virus phylogeny, ct values and without any description if and how containment measurements were followed under lock-down conditions. Although being performed at a hotspot, PCR results are not particular exciting. 439/12597=3.4% as measured by official surveillance and 33/919=3.6% as measured by the authors.
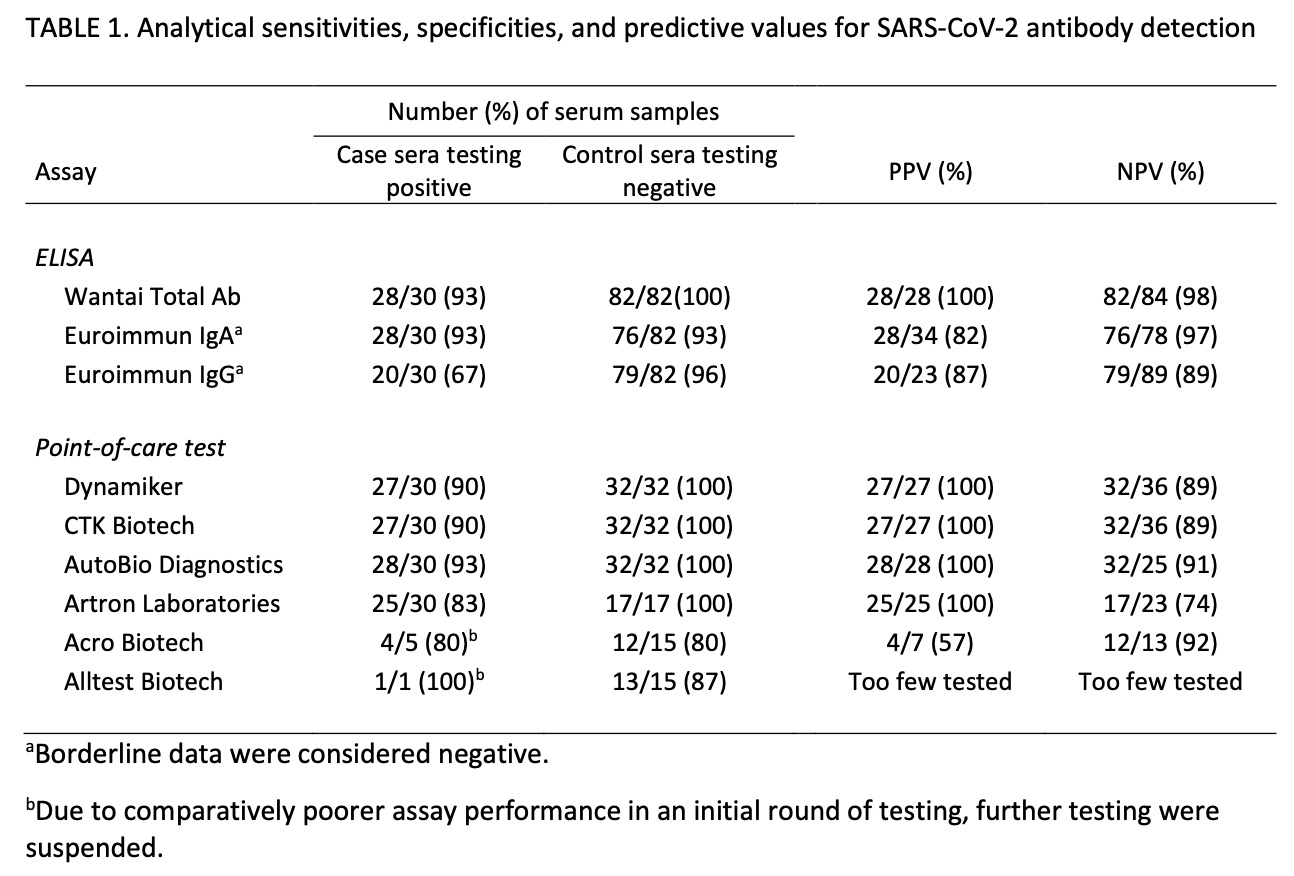
The claim to fame (besides some annoying reports about the accompanying PR campaign that made it even into Science magazine) are those 15% antibody positive results. Everything in this paper depends on the IgG antibody specificity to Sars-Cov2. It is reported
as of April 7, 2020, validated in cooperation with the Institute of Virology of the Charité in Berlin, and the Erasmus MC in Rotterdam, Euroimmun, Lübeck, Germany). The data sheet (April 7, 2020) reports cross-reactivities with anti-SARS-CoV-1-IgG-antibodies, but not with MERS-CoV-, HCoV-229E-, HCoV-NL63-, HCoV-HKU1- or HCoV-OC43-IgG antibodies.
Interestingly this data sheet was produced only after the examination. I could neither obtain it per email nor is it available on the manufacturer’s website. I also do not understand why Drosten criticized Streeck for this assay. Wasn’t he involved in the validation?
Here is how the authors checked their own methods

which is a bit weak regarding current pre-test standards, neither in terms of selection of samples, numbers and reporting. The press briefing even adds more confusion

as this reference is not cited in the preprint. I assume it is the Lassaunière comparison (medRxiv preprint) that showed a specificity of 96% only which is n o t s o good with the low prevalence expected.
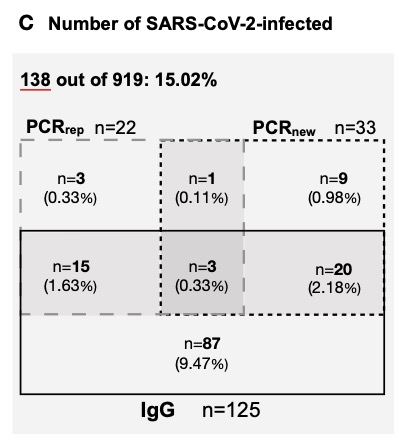
A further study on medRxiv reported a specificity of 99% using a “well-defined specificity panel of 147 serum and plasma samples” without any further description. Seroconversion data would also been helpful from Gangelt – why are those N=9 in the figure below not being retested after 2 weeks?
In the absence of any hard data the results remains questionable although it shouldn’t be impossible to design and validate a reliable test where even ultra-sensitive assays have been already published.
Why haven’t the neutralisation tests been incorporated?
Lets step into the results.
“PCRreported” overlaps with “PCRnew” as expected while I would like to see also the match of PCRnew with PCRreported negative results.
– the preliminary case fatality CFR was 0.37% based on 7 individuals. This figure remained unchanged even when moving to infection fatality IFR that should be lower as the denominator increased with more infections. Patients also continued to die after the end of the observation period, making the IFR estimate unreliable if not expanded by the 14-21 day usual symptom to death interval.
I tried to validate those 7 deaths reported in the manuscript for Gangelt until March 30. RKI reports 55 in the district Heinsberg until March 30. Did most of them really happen outside Gangelt?
According to the official statistics of the state department we may expect 11 deaths per month in Gangelt. So with the 7 reported cases we should find 18 cases by the end of March. According to the website https://www.aachen-gedenkt.de there are, however, 21 obituaries found in Gangelt eg 3 more than expected. Maybe there are some errors in my re-analysis as the obituaries do not always give the last address or not each death results in an obituary but we can assume that there was at least an excess of 10 and not only of 7 cases until March 30. For a final estimate we need to add at least 1 more case who died after the end of study. My estimate therefore is at least 11 and not just 7 cases.
– Why have the death certificates not been verified in a paper that has even “infection fatality rate” in the title?
– Why are there no virus tests in the victims?

6.5.2020 UPDATE
Sahm / FAZ complained about the confidence interval.
The current IFR in the USA is not 0.36% but 1.3% (95% CI: 0.6% to 2.1%) with county-specific rates varied from 0.5% to 3.6% according to Basu 2020. With a correct figure of 11 deaths out of 15/100 * 12.000 in Gangelt, the IFR is 0,61% and compatible with the lower end of the US distribution,
11.5.2020 UPDATE
mortality figure Heinsberg / Gangelt
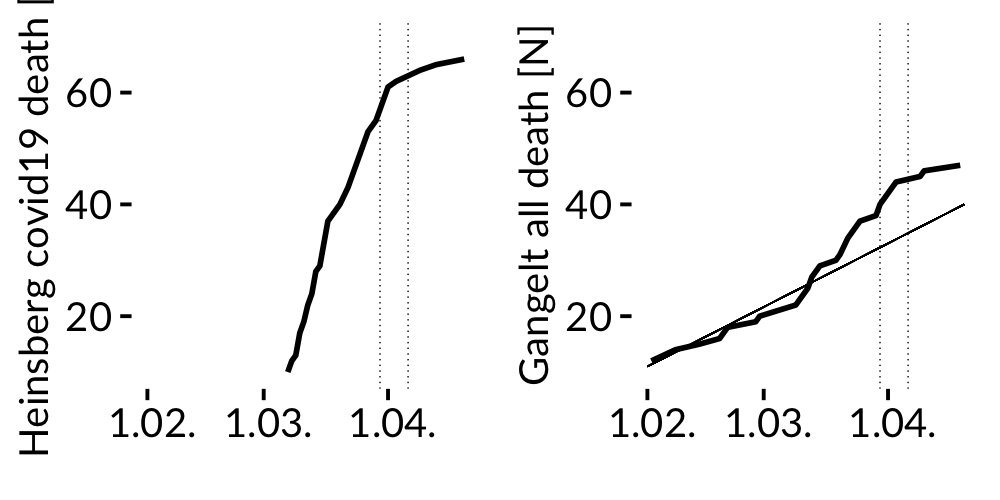

According to official RKI data about 15% of all Covid-19 related deaths in the district occurred in Gangelt although only 5% of the population of the Heinsberg district is living there.
The average all cause death in Gangelt doubled in March when compared to years 2000-2018.
Summary: The excess number of deaths in Gangelt by the end of the study is much higher than reported in the manuscript.