CC-BY-NC Science Surf , accessed 10.08.2026
Vier Jahre Vorlauf, ein Anhörungstermin der Enquete Kommission, und am Ende steht der Satz, der seit 2020 jede unbequeme Frage zuverlässig entsorgt: dazu brauche es mehr Forschung.
Die Wirksamkeit der NPIs bleibt offen, dafür ist die Zuständigkeit für das Offenbleiben jetzt sauber dokumentiert. Immerhin schreibt sich “Epidemologin” schneller als das Wort mit i; der LMU Vorgänger der Epidemiologin hatte den Corona-Leugnern ohnehin schon den Hof gemacht. Man arbeitet also weiter an der Anschlussfähigkeit.
Epidemologin Prof. Dr. Eva Annette Rehfuess von der Ludwig-Maximilians-Universität München wies jedoch am Beispiel des Maskentragens auf soziokulturelle Unterschiede zwischen Deutschland und Skandinavien hin…
Schutzmaßnahmen können auch Schaden anrichten. Rehfuess nannte es "nur bedingt sinnvoll", auf die Wirksamkeit einzelner Eindämmungsmaßnahmen zu sehen. Entscheidend sei immer ein Maßnahmenbündel. NPIs könnten schützen, sie könnten aber auch Schaden anrichten. Als Beispiel nannte sie die Schulschließungen, die bei vielen Kindern und Jugendlichen zu psychischen und sozialen, aber auch gesundheitlichen Schäden geführt haben. Insgesamt seien solche Nebenwirkungen während der Corona-Pandemie "zu wenig beforscht" worden, befand Rehfuess: "Da müssen wir in Zukunft früher ran."

Natürlich ist es sinnvoll, NPI einzeln und in Kombination zu untersuchen – da gab es genügend Forschung auch in Deutschland, die Wikipedia hat eine gute Übersicht. Ob man dabei den Schweden wirklich folgen will, die sich selbst bei COVID so blamiert haben? Aber man kann sich ja aus den tausenden Einzelstudien selbst heraus suchen, an was man am liebsten glauben möchte.
Oder mehr Forschung fordern.
In seinen “Empfehlungen für die Hochschulbildung in Zeiten generativer KI” plädiert der WR für “Intellektuelle Souveränität” als Leitidee, die den Hochschulen und allen beteiligten Akteursgruppen Orientierung bieten und für den Umgang mit generativer KI leitend sein soll. Gefordert seien Autonomie im Sinne von Selbstbestimmung, epistemischer Eigenständigkeit und Gerechtigkeit, kritische Reflexion und Widerstand gegen “bequeme Vereinfachung”.
Schön, daß wir uns weiterhin kritisch äussern sollen. Es wird nicht einfach sein.
These are my questions when reading the Nature news article although it has a quite different title “Think preprints are unreliable? Analysis of 70,000 studies might change your mind”.
The central conclusions of biomedical preprints rarely change following peer review in a journal, according to a study posted on the preprint server bioRxiv this month. The research also found that studies that appeared first as preprints are retracted at roughly half the rate of papers that did not appear online before being in a peer-reviewed journal. The authors say the findings suggests that preprints are a reliable source of information, although some scientists say the finding should be interpreted more cautiously.
It is all about this preprint
The primary claim was unchanged in 39.9% of abstracts, minorly revised in 50.0%, and substantially revised in only 10.2%.
Fits my experience.
There is a new bioRxiv preprint examining traditional peer review that is slowed by delays finding reviewers and waiting for reports.
In 2025, Biology Open expanded its Fast & Fair peer review model, using pre-contracted, paid reviewers (£220 or 250€ per manuscript, paid only for timely, quality reviews) with a structured editorial timeline. The program cut time to first decision from 38 to 6 working days, and improved reviewer commitment: higher acceptance (67% vs 23%) and higher completion (98% vs 87%). Review quality and acceptance rates were unchanged.
So it is overdue to replace ad hoc reviewer recruitment with paid, deadline-driven, quality-contingent review.
Die Meinungen darüber gehen auseinander.
Zwei Gastbeiträge von Ministerin Katherina Reiche unter KI-Verdacht – ob das nun von einem Lobbyisten, einem Redenschreiber einer KI oder etwa der Ministerin verfasst wurde, macht in dem Fall keinen großen Unterschied – es wird immer gleich defizitär sein.
Allerdings teile ich nicht die Meinung des SPIEGEL, der sich auf die Analyse Tools verlässt – zu sehr manipulierbar, zu sehr fehleranfällig.
Pangram und GPTZero kommen übereinstimmend zu dem Ergebnis, dass diese Worte mit hoher Wahrscheinlichkeit von einer künstlichen Intelligenz geschrieben wurden… Bei einer Nachprüfung des SPIEGEL berechnete das Werkzeug, dass nur die ersten 29 Prozent von einem Menschen geschrieben wurden.
Zur Illusion muss man einfach nur den Prompt bei der letzten Revision ändern auf “lass es nicht wie AI aussehen” und die üblichen KI Sonderzeichen entfernen.
Ich schliesse mich dafür lieber den Journalistenverbänden an, die eine Kennzeichnungspflicht für KI-Inhalte fordern – ganz im Unterschied zum deutschen Presserat.
Der Deutsche Presserat spricht sich in der aktuellen Diskussion über künstliche Intelligenz in den Medien gegen eine generelle Kennzeichnungspflicht aus…
Die Journalistenverbände DJV und dju haben beide eine Kennzeichnungspflicht für journalistische Beiträge gefordert … Dies solle im Pressekodex verankert werden …
»Die aktuelle Diskussion über künstliche Intelligenz in journalistischen Texten zeigt, dass die Glaubwürdigkeit des Journalismus auf dem Spiel steht«, erklärte der DJV-Bundesvorsitzende Mika Beuster. …
KI könne, etwa bei der Recherche, ein hilfreiches Werkzeug für Medienschaffende sein. Journalistinnen und Journalisten müssten hier aber klipp und klar Farbe bekennen.
Ich versuche dazu mal eine Klassifikation aus meiner Praxis
Der Text hier is KI:0.
Weiterlesen zum Thema bei Übermedien
Der berühmte "human in the loop" also, der Mensch, der noch mal kontrolliert und entscheidet, was online geht … Wie präzise diese Kontrollen dann sind oder ob sie überhaupt stattfinden, ist oft fraglich… "Autorschaft ist gekoppelt an Identität und Verantwortung", schreibt der Journalistik-Professor Tanjev Schultz in seiner aktuellen Kolumne über KI-Täuschungen im Journalismus.
Ein Machtwort: Wir schreiben selbs! https://www.spiegel.de/politik/kuenstliche-intelligenz-wie-der-spiegel-ki-in-der-redaktion-einsetzt-a-51cbb6aa-4bcc-4a9d-a70a-fc9df37e0611
Nicht minder wichtig: Massenmodelle sind etwas für die Massen! https://beimwort.substack.com/p/das-hier-ware-fast-ein-anti-ki-manifest?r=359c7u&utmmedium=ios&triedRedirect=true
Without doubt, the new Leiden Declaration on AI use is a clear step forward.
Without doubt, scientific results are always attributable to specific authors who take credit for their discovery and assume also responsibility.
Without doubt, revising my text by an AI (adding occasionally a point or removing one for being unqualified) benefits my programming and writing.
So AI support is indicated now not only in all recent papers but also for blog entries since March 2026.
As AI models are trained on vast amounts of text, including published, polished prose that uses professional typesetting, which is why they default to these more precise characters although they cannot be simply reached by a keyboard. Some examples are
A forensic caveat: these are heuristics, not proof. Smart-punctuation in any word processor produces identical glyphs from human input, and a model can be told to emit ASCII. The presence raises the prior; it does not establish AI provenance.
/* glyph-highlighter bookmarklet - add the following single line as a bookmark */
javascript:(function(){var ID='glyphHL',ex=document.querySelectorAll('mark.'+ID);if(ex.length){ex.forEach(function(m){m.replaceWith(document.createTextNode(m.dataset.c))});document.body.normalize();['_'+ID+'s','_'+ID+'b'].forEach(function(i){var e=document.getElementById(i);if(e)e.remove()});return}var G={'\u2014':['em dash','U+2014','dash'],'\u2013':['en dash','U+2013','dash'],'\u2212':['minus','U+2212','dash'],'\u2010':['hyphen','U+2010','dash'],'\u2012':['figure dash','U+2012','dash'],'\u2015':['horizontal bar','U+2015','dash'],'\u201C':['left double quote','U+201C','quote'],'\u201D':['right double quote','U+201D','quote'],'\u2018':['left single quote','U+2018','quote'],'\u2019':['apostrophe / right single','U+2019','quote'],'\u2032':['prime','U+2032','quote'],'\u2033':['double prime','U+2033','quote'],'\u2026':['ellipsis','U+2026','ell'],'\u00A0':['no-break space','U+00A0','space','NB'],'\u2009':['thin space','U+2009','space','TH'],'\u202F':['narrow nbsp','U+202F','space','NNB'],'\u200C':['zero-width non-joiner','U+200C','space','ZWNJ'],'\u200D':['zero-width joiner','U+200D','space','ZWJ'],'\uFEFF':['BOM / zwnbsp','U+FEFF','space','BOM']};var cls='[\\u2014\\u2013\\u2212\\u2010\\u2012\\u2015\\u201C\\u201D\\u2018\\u2019\\u2032\\u2033\\u2026\\u00A0\\u2009\\u202F\\u200C\\u200D\\uFEFF]';var has=new RegExp(cls),rx=new RegExp(cls,'g');var s=document.createElement('style');s.id='_'+ID+'s';s.textContent='mark.'+ID+'{border-radius:2px;padding:0 1px;color:inherit;box-shadow:0 0 0 1px rgba(0,0,0,.2)}mark.'+ID+'.dash{background:#bcd0ff}mark.'+ID+'.quote{background:#ecc9ff}mark.'+ID+'.ell{background:#b8efe2}mark.'+ID+'.space{background:#ffd0c4;outline:1px dashed #b23b2e;display:inline-block;min-width:.5em;text-align:center}mark.'+ID+'.space::after{content:attr(data-x);font:9px/1 monospace;color:#b23b2e;vertical-align:super;margin-left:1px}';document.head.appendChild(s);var c={dash:0,quote:0,ell:0,space:0},nodes=[],w=document.createTreeWalker(document.body,NodeFilter.SHOW_TEXT,{acceptNode:function(n){if(!n.nodeValue||!has.test(n.nodeValue))return 3;var p=n.parentNode,t=p&&p.nodeName;if(t=='SCRIPT'||t=='STYLE'||t=='NOSCRIPT'||t=='TEXTAREA')return 3;if(p&&p.isContentEditable)return 3;return 1}});while(w.nextNode())nodes.push(w.currentNode);nodes.forEach(function(n){var f=document.createDocumentFragment(),v=n.nodeValue,last=0,m;rx.lastIndex=0;while((m=rx.exec(v))){var ch=m[0],i=m.index,g=G[ch];if(i>last)f.appendChild(document.createTextNode(v.slice(last,i)));var mk=document.createElement('mark');mk.className=ID+' '+g[2];mk.dataset.c=ch;mk.title=g[0]+' '+g[1];if(g[2]=='space')mk.dataset.x=g[3];mk.textContent=ch;f.appendChild(mk);c[g[2]]++;last=i+ch.length}if(last<v.length)f.appendChild(document.createTextNode(v.slice(last)));n.parentNode.replaceChild(f,n)});var tot=c.dash+c.quote+c.ell+c.space,b=document.createElement('div');b.id='_'+ID+'b';b.style.cssText='position:fixed;z-index:2147483647;right:12px;bottom:12px;background:#14161a;color:#fff;font:12px/1.5 system-ui,sans-serif;padding:8px 12px;border-radius:6px;box-shadow:0 2px 10px rgba(0,0,0,.3);max-width:240px';b.innerHTML='<b>'+tot+'</b> typeset glyphs<br>'+c.dash+' dash · '+c.quote+' quote · '+c.ell+' ellipsis · '+c.space+' space/hidden<br><span style="opacity:.7">click the bookmarklet again to clear</span>';document.body.appendChild(b)})();
/* glyph-highlighter bookmarklet - readable source
*
* Highlights typeset Unicode glyphs that a plain keyboard does not produce.
* Run once to highlight; run again on the same page to remove.
*
* Categories (CSS class + colour):
* dash blue em/en/minus/hyphen/figure dash/horizontal bar
* quote purple curly quotes, curly apostrophe, prime, double prime
* ell teal ellipsis
* space red, dashed no-break/thin/narrow spaces + zero-width chars (ZWJ/ZWNJ/BOM)
*
* Invisible characters carry a small superscript tag (NB, TH, ZWJ, ...) via ::after,
* because they have no visible shape of their own.
*
* To install: minify to a single line and prefix with "javascript:" as a bookmark URL,
* or use the one-liner already provided.
*/
(function () {
var ID = 'glyphHL';
// --- toggle off: if marks exist, unwrap them and remove injected nodes ---
var existing = document.querySelectorAll('mark.' + ID);
if (existing.length) {
existing.forEach(function (m) {
m.replaceWith(document.createTextNode(m.dataset.c)); // restore original char
});
document.body.normalize(); // merge split text nodes back together
['_' + ID + 's', '_' + ID + 'b'].forEach(function (id) {
var el = document.getElementById(id);
if (el) el.remove();
});
return;
}
// --- glyph table: char -> [name, codepoint, category, shortTag?] ---
var G = {
'\u2014': ['em dash', 'U+2014', 'dash'],
'\u2013': ['en dash', 'U+2013', 'dash'],
'\u2212': ['minus', 'U+2212', 'dash'],
'\u2010': ['hyphen', 'U+2010', 'dash'],
'\u2012': ['figure dash', 'U+2012', 'dash'],
'\u2015': ['horizontal bar', 'U+2015', 'dash'],
'\u201C': ['left double quote', 'U+201C', 'quote'],
'\u201D': ['right double quote', 'U+201D', 'quote'],
'\u2018': ['left single quote', 'U+2018', 'quote'],
'\u2019': ['apostrophe / right single', 'U+2019', 'quote'],
'\u2032': ['prime', 'U+2032', 'quote'],
'\u2033': ['double prime', 'U+2033', 'quote'],
'\u2026': ['ellipsis', 'U+2026', 'ell'],
'\u00A0': ['no-break space', 'U+00A0', 'space', 'NB'],
'\u2009': ['thin space', 'U+2009', 'space', 'TH'],
'\u202F': ['narrow no-break space', 'U+202F', 'space', 'NNB'],
'\u200C': ['zero-width non-joiner', 'U+200C', 'space', 'ZWNJ'],
'\u200D': ['zero-width joiner', 'U+200D', 'space', 'ZWJ'],
'\uFEFF': ['BOM / zero-width no-break space', 'U+FEFF', 'space', 'BOM']
};
// character class covering every key above
var cls = '[\\u2014\\u2013\\u2212\\u2010\\u2012\\u2015\\u201C\\u201D\\u2018\\u2019' +
'\\u2032\\u2033\\u2026\\u00A0\\u2009\\u202F\\u200C\\u200D\\uFEFF]';
var has = new RegExp(cls); // non-global: safe for .test()
var rx = new RegExp(cls, 'g'); // global: used to scan/split text
// --- injected stylesheet ---
var style = document.createElement('style');
style.id = '_' + ID + 's';
style.textContent =
'mark.' + ID + '{border-radius:2px;padding:0 1px;color:inherit;box-shadow:0 0 0 1px rgba(0,0,0,.2)}' +
'mark.' + ID + '.dash{background:#bcd0ff}' +
'mark.' + ID + '.quote{background:#ecc9ff}' +
'mark.' + ID + '.ell{background:#b8efe2}' +
'mark.' + ID + '.space{background:#ffd0c4;outline:1px dashed #b23b2e;display:inline-block;min-width:.5em;text-align:center}' +
'mark.' + ID + '.space::after{content:attr(data-x);font:9px/1 monospace;color:#b23b2e;vertical-align:super;margin-left:1px}';
document.head.appendChild(style);
// --- collect candidate text nodes ---
var counts = { dash: 0, quote: 0, ell: 0, space: 0 };
var nodes = [];
var walker = document.createTreeWalker(document.body, NodeFilter.SHOW_TEXT, {
acceptNode: function (n) {
if (!n.nodeValue || !has.test(n.nodeValue)) return NodeFilter.FILTER_REJECT;
var p = n.parentNode, t = p && p.nodeName;
if (t === 'SCRIPT' || t === 'STYLE' || t === 'NOSCRIPT' || t === 'TEXTAREA') return NodeFilter.FILTER_REJECT;
if (p && p.isContentEditable) return NodeFilter.FILTER_REJECT;
return NodeFilter.FILTER_ACCEPT;
}
});
while (walker.nextNode()) nodes.push(walker.currentNode);
// --- wrap each matched glyph ---
nodes.forEach(function (n) {
var frag = document.createDocumentFragment();
var v = n.nodeValue, last = 0, m;
rx.lastIndex = 0;
while ((m = rx.exec(v))) {
var ch = m[0], i = m.index, g = G[ch];
if (i > last) frag.appendChild(document.createTextNode(v.slice(last, i)));
var mk = document.createElement('mark');
mk.className = ID + ' ' + g[2];
mk.dataset.c = ch; // original char, for clean restore
mk.title = g[0] + ' ' + g[1]; // hover tooltip: name + codepoint
if (g[2] === 'space') mk.dataset.x = g[3];
mk.textContent = ch;
frag.appendChild(mk);
counts[g[2]]++;
last = i + ch.length;
}
if (last < v.length) frag.appendChild(document.createTextNode(v.slice(last)));
n.parentNode.replaceChild(frag, n);
});
// --- count badge ---
var total = counts.dash + counts.quote + counts.ell + counts.space;
var badge = document.createElement('div');
badge.id = '_' + ID + 'b';
badge.style.cssText =
'position:fixed;z-index:2147483647;right:12px;bottom:12px;background:#14161a;color:#fff;' +
'font:12px/1.5 system-ui,sans-serif;padding:8px 12px;border-radius:6px;' +
'box-shadow:0 2px 10px rgba(0,0,0,.3);max-width:240px';
badge.innerHTML =
'<b>' + total + '</b> typeset glyphs<br>' +
counts.dash + ' dash \u00B7 ' + counts.quote + ' quote \u00B7 ' +
counts.ell + ' ellipsis \u00B7 ' + counts.space + ' space/hidden<br>' +
'<span style="opacity:.7">click the bookmarklet again to clear</span>';
document.body.appendChild(badge);
})();
And here is already v2 – using a word list from a new PNAS paper by
/* ai-highlighter bookmarklet - add the following single line as a bookmark */
javascript:(function(){var ID='glyphHL',ex=document.querySelectorAll('mark.'+ID);if(ex.length){ex.forEach(function(m){m.replaceWith(document.createTextNode(m.dataset.c))});document.body.normalize();['_'+ID+'s','_'+ID+'b'].forEach(function(i){var e=document.getElementById(i);if(e)e.remove()});return}var G={'-':['em dash','U+2014','dash'],'-':['en dash','U+2013','dash'],'-':['minus','U+2212','dash'],'-':['hyphen','U+2010','dash'],'-':['figure dash','U+2012','dash'],'-':['horizontal bar','U+2015','dash'],'"':['left double quote','U+201C','quote'],'"':['right double quote','U+201D','quote'],''':['left single quote','U+2018','quote'],''':['apostrophe / right single','U+2019','quote'],''':['prime','U+2032','quote'],'"':['double prime','U+2033','quote'],'...':['ellipsis','U+2026','ell'],' ':['no-break space','U+00A0','space','NB'],' ':['thin space','U+2009','space','TH'],' ':['narrow nbsp','U+202F','space','NNB'],'':['zero-width non-joiner','U+200C','space','ZWNJ'],'':['zero-width joiner','U+200D','space','ZWJ'],'':['BOM / zwnbsp','U+FEFF','space','BOM']};var WSET=Object.create(null);('achieves achieving acknowledges adaptable addressing adept adeptly adjustments adjusts advancements advancing advocating aiding align aligning aligns alongside amidst amplifies avenues boasting boasts bolster bolstering bolsters broader capitalizes captivating captures capturing categorizes categorizing commendable complexities complicates complicating compromising consolidates contextualize contextually cornerstone crucial culminating delineates delve delved delves delving dependencies diminishes discernible downturns dynamically elucidates elucidating emphasising emphasizes emphasizing employs enabling encapsulates encompass encompassed encompasses encompassing endeavors enhance enhancements enhances enhancing ensures ensuring equipping equips escalate escalating exacerbates exacerbating exceeding excelled excelling excels exemplifies exhibits facilitating featuring formidable fortifying fostering fosters foundational frameworks garnered garnering grappling groundbreaking harnessing heighten heightened heightening heightens highlighting highlights hinges imperatives inadequately inadvertently incentivizes incentivizing incorporates incorporating inefficiencies inherently insights integrates integrating intensifies intensifying interpretability interpretable intricacies intricacy intricate intricately introduces juncture leverage leverages leveraging meticulous meticulously mitigate mitigates mitigating multifaceted navigates navigating necessitate necessitates necessitating notable notably nuanced nuances offering offers outperforming overlook overlooking overlooks overreliance overseeing oversight oversimplify paving pinpointing pivotal poised posits practicality preserving primarily prioritise prioritize prioritizes prioritizing promise prowess reaffirming realm redefines refine refines refining reflecting reinforces reliance renowned reshapes reshaping revolutionize revolutionizing rigor safeguard safeguarding safeguards seamless seamlessly serves showcases showcasing signifying situates situating sourced strategically streamline streamlined streamlining strengthens struggle stylistic surpasses surpassing symbolizing synthesizes thereby thoroughness thoughtfully thrives timelines transcends transitioning underexplored undermines underperform underperformed underpins underscore underscored underscores underscoring unlock unlocking utilizes validates warranting workflows').split(' ').forEach(function(w){WSET[w]=1});var gc='[\\u2014\\u2013\\u2212\\u2010\\u2012\\u2015\\u201C\\u201D\\u2018\\u2019\\u2032\\u2033\\u2026\\u00A0\\u2009\\u202F\\u200C\\u200D\\uFEFF]';var has=new RegExp(gc+'|[A-Za-z]{4,}'),rx=new RegExp(gc+'|[A-Za-z]{4,}','g');var s=document.createElement('style');s.id='_'+ID+'s';s.textContent='mark.'+ID+'{border-radius:2px;padding:0 1px;color:inherit;box-shadow:0 0 0 1px rgba(0,0,0,.2)}mark.'+ID+'.dash{background:#bcd0ff}mark.'+ID+'.quote{background:#ecc9ff}mark.'+ID+'.ell{background:#b8efe2}mark.'+ID+'.word{background:#ffe680}mark.'+ID+'.space{background:#ffd0c4;outline:1px dashed #b23b2e;display:inline-block;min-width:.5em;text-align:center}mark.'+ID+'.space::after{content:attr(data-x);font:9px/1 monospace;color:#b23b2e;vertical-align:super;margin-left:1px}';document.head.appendChild(s);var c={dash:0,quote:0,ell:0,space:0,word:0},nodes=[],w=document.createTreeWalker(document.body,NodeFilter.SHOW_TEXT,{acceptNode:function(n){if(!n.nodeValue||!has.test(n.nodeValue))return 3;var p=n.parentNode,t=p&&p.nodeName;if(t=='SCRIPT'||t=='STYLE'||t=='NOSCRIPT'||t=='TEXTAREA')return 3;if(p&&p.isContentEditable)return 3;return 1}});while(w.nextNode())nodes.push(w.currentNode);nodes.forEach(function(n){var f=document.createDocumentFragment(),v=n.nodeValue,last=0,m,hit=false;rx.lastIndex=0;while((m=rx.exec(v))){var tok=m[0],i=m.index,g=G[tok],cat,tag;if(g){cat=g[2];if(cat=='space')tag=g[3]}else{if(!WSET[tok.toLowerCase()])continue;cat='word'}if(i>last)f.appendChild(document.createTextNode(v.slice(last,i)));var mk=document.createElement('mark');mk.className=ID+' '+cat;mk.dataset.c=tok;mk.title=g?g[0]+' '+g[1]:'focus word (Siler PNAS 2026)';if(tag)mk.dataset.x=tag;mk.textContent=tok;f.appendChild(mk);c[cat]++;last=i+tok.length;hit=true}if(!hit)return;if(last<v.length)f.appendChild(document.createTextNode(v.slice(last)));n.parentNode.replaceChild(f,n)});var gt=c.dash+c.quote+c.ell+c.space,b=document.createElement('div');b.id='_'+ID+'b';b.style.cssText='position:fixed;z-index:2147483647;right:12px;bottom:12px;background:#14161a;color:#fff;font:12px/1.5 system-ui,sans-serif;padding:8px 12px;border-radius:6px;box-shadow:0 2px 10px rgba(0,0,0,.3);max-width:260px';b.innerHTML='<b>'+gt+'</b> typeset glyphs · <b>'+c.word+'</b> focus words<br>'+c.dash+' dash · '+c.quote+' quote · '+c.ell+' ellipsis · '+c.space+' space/hidden<br><span style="opacity:.7">click the bookmarklet again to clear</span>';document.body.appendChild(b)})();
/* glyph + focus-word highlighter bookmarklet - readable source
*
* Highlights
* typeset Unicode glyphs a plain keyboard does not produce, and
* "focus words" - lexical tells of AI-generated prose from Siler et al.,
* PNAS 2026 (doi:10.1073/pnas.2605754123).
*
* Run once to highlight; run again on the same page to remove.
*
* Categories (CSS class + colour):
* dash blue em/en/minus/hyphen/figure dash/horizontal bar
* quote purple curly quotes, curly apostrophe, prime, double prime
* ell teal ellipsis
* space red, dashed no-break/thin/narrow spaces + zero-width chars
* word yellow Siler focus words (case-insensitive, whole word)
*
* Forensic caveat: these are heuristics, not proof. Smart-punctuation and
* ordinary academic vocabulary both produce identical output from human input.
* Presence raises the prior; it does not establish AI provenance.
*/
(function () {
var ID = 'glyphHL';
// --- toggle off: if marks exist, unwrap them and remove injected nodes ---
var existing = document.querySelectorAll('mark.' + ID);
if (existing.length) {
existing.forEach(function (m) {
m.replaceWith(document.createTextNode(m.dataset.c));
});
document.body.normalize();
['_' + ID + 's', '_' + ID + 'b'].forEach(function (id) {
var el = document.getElementById(id);
if (el) el.remove();
});
return;
}
// --- glyph table: char -> [name, codepoint, category, shortTag?] ---
var G = {
'-': ['em dash', 'U+2014', 'dash'],
'-': ['en dash', 'U+2013', 'dash'],
'-': ['minus', 'U+2212', 'dash'],
'-': ['hyphen', 'U+2010', 'dash'],
'-': ['figure dash', 'U+2012', 'dash'],
'-': ['horizontal bar', 'U+2015', 'dash'],
'"': ['left double quote', 'U+201C', 'quote'],
'"': ['right double quote', 'U+201D', 'quote'],
''': ['left single quote', 'U+2018', 'quote'],
''': ['apostrophe / right single', 'U+2019', 'quote'],
''': ['prime', 'U+2032', 'quote'],
'"': ['double prime', 'U+2033', 'quote'],
'...': ['ellipsis', 'U+2026', 'ell'],
' ': ['no-break space', 'U+00A0', 'space', 'NB'],
' ': ['thin space', 'U+2009', 'space', 'TH'],
' ': ['narrow no-break space', 'U+202F', 'space', 'NNB'],
'': ['zero-width non-joiner', 'U+200C', 'space', 'ZWNJ'],
'': ['zero-width joiner', 'U+200D', 'space', 'ZWJ'],
'': ['BOM / zero-width no-break space', 'U+FEFF', 'space', 'BOM']
};
// --- Siler focus words (PNAS 2026), lowercase, stored in a Set for O(1) lookup ---
var WORDS = ('achieves achieving acknowledges adaptable addressing adept adeptly ' +
'adjustments adjusts advancements advancing advocating aiding align aligning ' +
'aligns alongside amidst amplifies avenues boasting boasts bolster bolstering ' +
'bolsters broader capitalizes captivating captures capturing categorizes ' +
'categorizing commendable complexities complicates complicating compromising ' +
'consolidates contextualize contextually cornerstone crucial culminating ' +
'delineates delve delved delves delving dependencies diminishes discernible ' +
'downturns dynamically elucidates elucidating emphasising emphasizes ' +
'emphasizing employs enabling encapsulates encompass encompassed encompasses ' +
'encompassing endeavors enhance enhancements enhances enhancing ensures ' +
'ensuring equipping equips escalate escalating exacerbates exacerbating ' +
'exceeding excelled excelling excels exemplifies exhibits facilitating ' +
'featuring formidable fortifying fostering fosters foundational frameworks ' +
'garnered garnering grappling groundbreaking harnessing heighten heightened ' +
'heightening heightens highlighting highlights hinges imperatives inadequately ' +
'inadvertently incentivizes incentivizing incorporates incorporating ' +
'inefficiencies inherently insights integrates integrating intensifies ' +
'intensifying interpretability interpretable intricacies intricacy intricate ' +
'intricately introduces juncture leverage leverages leveraging meticulous ' +
'meticulously mitigate mitigates mitigating multifaceted navigates navigating ' +
'necessitate necessitates necessitating notable notably nuanced nuances ' +
'offering offers outperforming overlook overlooking overlooks overreliance ' +
'overseeing oversight oversimplify paving pinpointing pivotal poised posits ' +
'practicality preserving primarily prioritise prioritize prioritizes ' +
'prioritizing promise prowess reaffirming realm redefines refine refines ' +
'refining reflecting reinforces reliance renowned reshapes reshaping ' +
'revolutionize revolutionizing rigor safeguard safeguarding safeguards ' +
'seamless seamlessly serves showcases showcasing signifying situates situating ' +
'sourced strategically streamline streamlined streamlining strengthens ' +
'struggle stylistic surpasses surpassing symbolizing synthesizes thereby ' +
'thoroughness thoughtfully thrives timelines transcends transitioning ' +
'underexplored undermines underperform underperformed underpins underscore ' +
'underscored underscores underscoring unlock unlocking utilizes validates ' +
'warranting workflows').split(' ');
var WSET = Object.create(null);
WORDS.forEach(function (w) { WSET[w] = 1; });
// --- combined matcher: any glyph char OR a run of ASCII letters (>=4) ---
var glyphCls = '[\\u2014\\u2013\\u2212\\u2010\\u2012\\u2015\\u201C\\u201D\\u2018\\u2019' +
'\\u2032\\u2033\\u2026\\u00A0\\u2009\\u202F\\u200C\\u200D\\uFEFF]';
var has = new RegExp(glyphCls + '|[A-Za-z]{4,}');
var rx = new RegExp(glyphCls + '|[A-Za-z]{4,}', 'g');
// --- injected stylesheet ---
var style = document.createElement('style');
style.id = '_' + ID + 's';
style.textContent =
'mark.' + ID + '{border-radius:2px;padding:0 1px;color:inherit;box-shadow:0 0 0 1px rgba(0,0,0,.2)}' +
'mark.' + ID + '.dash{background:#bcd0ff}' +
'mark.' + ID + '.quote{background:#ecc9ff}' +
'mark.' + ID + '.ell{background:#b8efe2}' +
'mark.' + ID + '.word{background:#ffe680}' +
'mark.' + ID + '.space{background:#ffd0c4;outline:1px dashed #b23b2e;display:inline-block;min-width:.5em;text-align:center}' +
'mark.' + ID + '.space::after{content:attr(data-x);font:9px/1 monospace;color:#b23b2e;vertical-align:super;margin-left:1px}';
document.head.appendChild(style);
// --- collect candidate text nodes ---
var counts = { dash: 0, quote: 0, ell: 0, space: 0, word: 0 };
var nodes = [];
var walker = document.createTreeWalker(document.body, NodeFilter.SHOW_TEXT, {
acceptNode: function (n) {
if (!n.nodeValue || !has.test(n.nodeValue)) return NodeFilter.FILTER_REJECT;
var p = n.parentNode, t = p && p.nodeName;
if (t === 'SCRIPT' || t === 'STYLE' || t === 'NOSCRIPT' || t === 'TEXTAREA') return NodeFilter.FILTER_REJECT;
if (p && p.isContentEditable) return NodeFilter.FILTER_REJECT;
return NodeFilter.FILTER_ACCEPT;
}
});
while (walker.nextNode()) nodes.push(walker.currentNode);
// --- wrap each matched glyph or focus word ---
nodes.forEach(function (n) {
var frag = document.createDocumentFragment();
var v = n.nodeValue, last = 0, m, hit = false;
rx.lastIndex = 0;
while ((m = rx.exec(v))) {
var tok = m[0], i = m.index, g = G[tok], cat, tag;
if (g) { // a typeset glyph
cat = g[2];
if (cat === 'space') tag = g[3];
} else { // a letter run - is it a focus word?
if (!WSET[tok.toLowerCase()]) continue; // not on the list: leave as plain text
cat = 'word';
}
if (i > last) frag.appendChild(document.createTextNode(v.slice(last, i)));
var mk = document.createElement('mark');
mk.className = ID + ' ' + cat;
mk.dataset.c = tok; // original text, for clean restore
mk.title = g ? g[0] + ' ' + g[1] : 'focus word (Siler PNAS 2026)';
if (tag) mk.dataset.x = tag;
mk.textContent = tok;
frag.appendChild(mk);
counts[cat]++;
last = i + tok.length;
hit = true;
}
if (!hit) return;
if (last < v.length) frag.appendChild(document.createTextNode(v.slice(last)));
n.parentNode.replaceChild(frag, n);
});
// --- count badge ---
var glyphTotal = counts.dash + counts.quote + counts.ell + counts.space;
var badge = document.createElement('div');
badge.id = '_' + ID + 'b';
badge.style.cssText =
'position:fixed;z-index:2147483647;right:12px;bottom:12px;background:#14161a;color:#fff;' +
'font:12px/1.5 system-ui,sans-serif;padding:8px 12px;border-radius:6px;' +
'box-shadow:0 2px 10px rgba(0,0,0,.3);max-width:260px';
badge.innerHTML =
'<b>' + glyphTotal + '</b> typeset glyphs · <b>' + counts.word + '</b> focus words<br>' +
counts.dash + ' dash · ' + counts.quote + ' quote · ' +
counts.ell + ' ellipsis · ' + counts.space + ' space/hidden<br>' +
'<span style="opacity:.7">click the bookmarklet again to clear</span>';
document.body.appendChild(badge);
})();
Following the Lindau elogy there is a new Südhof paper in Neuroscience.
The biggest issue? Undisclosed self-interest. Südhof opens by admitting his own lab is under PubPeer scrutiny, then analyzes PubPeer as if providing neutral commentary. This is never adequately acknowledged as the primary driver of the piece. His attack on PubPeer commentors for income-dependent bias applies with greater force to himself.
The “income” claim misrepresents PubPeer’s structure. The assertion that PubPeer’s key proponents base their livelihood on comment success conflates a handful of individuals with the platform as a whole. PubPeer is a registered non-profit. The overwhelming majority of commentors are anonymous volunteers – I know only of a few exceptions Bik/Patreon, David/Dana Farber or Oransky/service fees. The characterization implies a structural commercial incentive that does not exist institutionally. Verdict – clearly wrong.
The Occam’s razor argument is logically invalid. He argues: if you wanted to fake a Western blot, you’d just load fake samples rather than manipulate images – therefore image manipulation is less likely. This is not my empirical experience: Image manipulation happens to rescue weak signals, fix failed loading controls, save time. The existence of an allegedly simpler path to fraud does not preclude the actual path taken. Applied consistently, this reasoning exculpates most detected fraud by construction.
“Minor issues with no bearing on main findings” is asserted without evidence. He repeats the Lindau argument as if established. The opposite is frequently documented: duplicated Western blots in result-critical panels, reused patient data across trials presented as independent cohorts, fabricated dose-response curves. No data are provided on PubPeer’s false positive rate, proportion of retractions later shown unjustified, or what fraction of flagged issues were peripheral vs. central to conclusions. Verdict – not a scientific argument
The proposed alternatives? Just a return control to the same failed system? eLife comments, Nature “Matters Arising”, and BioRxiv comments require formal authorship and pass through editorial gatekeeping by the same journals that sat on integrity concerns for years before PubPeer forced action. The history of that institutional failure is the reason PubPeer exists, and it goes entirely unaddressed.
Where Südhof is right. The description of the author-journal power imbalance is accurate and underappreciated. Journals recruit reviewers for free, make unilateral acceptance and retraction decisions, collect open-access fees, and provide authors no due process. A paper can be retracted without the authors having any formal right of appeal. COPE guidelines nominally govern this process but confer authority on journals, not authors.
(with AI support)
This story started by end of March 2026 – see also my arXiv preprint – with an email to the European Medical Association after examining some Iranian RCTs.
One of these was a teriparatide biosimilar that is under scrutinity by the EMA.
ASK-292796 – EMA Zandoriah / teriparatide received on 01/04/2026
Thank you for your message and your interest in the European Medicines Agency. Your request has been given the reference number ASK-292796.
Unfortunately there was no further response however.
So I repeated my email 6 weeks later
ASK-294576 – Zandoriah CHMP opinion received on 15/05/2026
Thank you for your message and your interest in the European Medicines Agency. Your request has been given the reference number ASK-294576.
We will reply to you as soon as we can. For complex queries, it may take longer to answer. In any case we will write back to you within 2 months from the date of receipt.
Please do not reply to this email, this is an automated response to confirm that we have received your request. If you need to contact us again about the same matter, please use the form on our website and mention the reference number.
Another 2 weeks later an EMA official (or an EMA bot) answered
The European Medicines Agency does not routinely request or receive individual patient-level datasets as part of its marketing authorisation applications. The Agency's evaluation is primarily based on the analyses and summaries provided by applicants, in line with the established regulatory framework. Please be informed that the European Public Assessment Report for this product will be published on the EMA website soon, it will contain the details of the assessment, including specific studies and types of data which served as the grounds for the CHMP Opinion.
With regards to your concerns raised, please note that we have a whistleblowing policy in place. Please check https://www.ema.europa.eu/en/about-us/how-we-work/external-whistleblowing-policy for further reference.
If you consider your concerns well-founded, you are welcome to submit full supporting and detailed evidence via the email reporting@ema.europa.eu so it can be properly assessed and acted upon as appropriate.
So I sent email number 3 to the reporting hotline.
Funnily, on the the next day, instead of a response, the EMA published numerous related Zandoriah documents including the anticipated market authorisation.
I am not an expert in reading these kind of official documents. Asking Claude for interpretation it says
A PK/PD comparability study was published but contains errors
The RMP (Module SII and SIII) names EudraCT 2019-004477-82 explicitly: an open-label, randomised, two-sequence, two-period crossover bioequivalence study in 60 healthy female subjects, comparing P044 20 µg vs Forsteo 20 µg single dose subcutaneous. This study has now been identified as Raykova et al. 2021 (Expert Opinion on Biological Therapy 22:2, 235-243) by CinnaGen employees and their contracted CRO in Bulgaria. The paper states that the study “was approved by independent ethical committee ” naming neither the committee nor its approval number or date, contrary to ICMJE requirements. For a study conducted in Sofia, Bulgaria by a CRO contracted by an Iranian sponsor, and submitted to EMA as part of a marketing authorisation dossier, the absence of independently verifiable ethics oversight documentation is a material reporting deficit.
The EMA report states 60 subjects; the published paper reports 66 enrolled, 56 completers, 48 PK-evaluable. The figure 60 probably corresponds to the P044 safety population (Table 5, N=60), suggesting the RMP cited the treatment-specific safety denominator rather than the enrolled N. The sample size section states CV=25%, 80% power, alpha=5% → n=56 required; standard TOST calculation for those inputs yields only n=16, not 56. Reverse engineering shows n=56 corresponds to an intrasubject CV of approximately 49%. Either the stated CV or the stated sample size is wrong.
Eight of 56 completers (14%) were excluded post-hoc from PK analysis for pre-dose concentrations exceeding 5% of Cmax. With a teriparatide half-life of approximately 1 hour and a 3-day washout, pharmacokinetic carryover is impossible. The paper investigated all plausible causes and found none. This cluster of unexplained pre-dose signals is almost certainly what the EMA’s provisional negative opinion referred to in September 2021 when it cited “uncertainties about the way results from the study on distribution in the body had been analysed.” The first EMA application (Teriparatide Cinnagen) was withdrawn on 9 September 2021, two weeks after this paper appeared online. The second application (Zandoriah) received a positive initial opinion in March 2026 although the arithmetic mean of t½ for P044 (0.95h, SD 1.80h) has SD exceeding mean, which is inconsistent with a normal distribution for a strictly positive variable and indicates severe right-skew or extreme outliers in the population.
If teriparatide PK differs between sexes (there is published evidence that it does as body weight, renal function, and volume of distribution differ systematically), then the bioequivalence demonstrated in healthy young women (mean age 33, mean BMI 24) may not extend to the male patients or older postmenopausal women who are the actual clinical population. This is a limitation of the design and would normally appear in the discussion. It does not.
The serum calcium PD endpoint used in this study reflects transient PTH receptor activation in kidney and gut, not the osteoblast stimulation and bone matrix formation that defines teriparatide’s clinical value, which operates over months and is measurable only through bone turnover markers or BMD.
Structural comparability data - peptide mapping, circular dichroism, receptor binding, cell-based bioassay - are absent from the published paper and the EPAR assessment report that would contain them remains unavailable. Eight of 56 completers (14.3%) had pharmacokinetically impossible pre-dose elevations despite a 72-half-life washout, most plausibly explained by ELISA cross-reactivity with endogenous PTH(1-84), which would mean the measured PK curves partially reflect endogenous hormone rather than the biosimilar. If assay specificity for P044 differs even slightly from that for Forsteo - due to differences in aggregation state or degradation profile - the apparent bioequivalence is an assay artefact,
The only clinical efficacy data in the entire dossier is the Tabatabaei-Malazy 2018 RCT that I identified in my paper.
The CinnoPar RCT (Tabatabaei-Malazy 2018) remains formally part of the dossier
The RMP Module SIII states it explicitly: 104 patients randomised, 94 analysed, 6-month follow-up. This is the study with documented impossible CVs, cross-variable mean duplicates, a CONSORT flow claiming zero exclusions despite extensive exclusion criteria, and a Table 1 denominator inconsistency (counts consistent with N=43, percentages consistent with N=44). EMA accepted this study as contributing to the clinical comparability claim. None of the documents address the data integrity issues documented on PubPeer.
The safety exposure is thin and the risk assessment is anomalous. Table 15 of the RMP states 52 patients exposed to CinnoPar across the entire clinical trial programme. The RMP then lists Important Identified Risks: None; Important Potential Risks: None; Missing Information: None. This triple “None” against a 52-patient safety database is a regulatory anomaly. The Forsteo originator dossier covered over 2,800 patients.
So EMA authorised Zandoriah on a dossier that includes: (1) a published bioequivalence study with unclear ethical provenance and a sample size calculation that is arithmetically irreconcilable with its stated inputs; (2) a clinical RCT with documented forensic anomalies that remain unaddressed in the regulatory record. (3) There is also currently no publicly verifiable basis for assessing whether P044/CinnoPar/Zandoriah is structurally and functionally comparable to Forsteo at the molecular level.
Following up a recent PubPeer post the journals integrity officer Dawn Peters wrote to me "You may submit a Perspective or letter to the editor". So I wrote this letter.
NEJM papers forming the empirical backbone of the hygiene hypothesis contain important methodological weaknesses. The journal's role was active rather than passive: the Bach 2002 review (1) and the accompanying editorial (2) were clear endorsements published alongside the first prominent farm/endotoxin findings. The hypothesis was rarely framed to allow falsification, and was repeatedly reformulated - from "infections" to "endotoxin" to "microbial diversity" to "innate immunity." Later disclosures of editorial conflicts of interest make a retrospective methodological audit overdue.
Bach (1), cited nearly 3,700 times, built its central argument on figures whose source data cannot be verified. Figure 1A cites a source containing seroprevalence rather than incidence data. Figure 1B assigns incorrect country categories. Figure 3 combines disease and economic data from sources that do not contain the values shown. Figure 4 relies on an unpublished personal communication that has not been replicated. The ecological framing throughout is insufficient to support causal inference.
Braun-Fahrländer (3) pools farming and non-farming children whose endotoxin exposures differ twofold into a single smoothed curve. The smoothing span is changed selectively for the one outcome contrary to the main hypothesis, without justification. Fewer than one third of eligible participants provided complete data, with no analysis of non-completers. After correction for multiple testing, virtually the entire Table 2 collapses to a single marginal result.
Ege (4) excluded wheeze-enriched children from the PARSIFAL sample, reducing wheeze prevalence from 8% to 3%, without disclosure in the main paper. In the resulting sample, the farm-asthma association is non-significant. The SSCP normalization standard contained the same organisms highlighted as the paper's headline protective finding. In the paper's own final model, the GABRIELA diversity result is null (OR 1.01, p=0.93) - neither value reported in the abstract.
Stein (5) infers genetic equivalence between Amish and Hutterite children from principal-component analysis of common SNPs, a method not suited to detecting the rare founder variants that distinguish these populations. Shared ancestry is thus not established, and the paper's central contrast - attributing the four-fold asthma difference to farming environment rather than genetic background - is not warranted.
These concerns - unverifiable source data, undisclosed sample exclusions, selective analytical choices, and abstracts that omit null results from the papers' own final models - are documented on PubPeer and remain unaddressed. Taken together, they indicate that the hygiene hypothesis was not established on sound empirical foundations.
I now received this response
Dear Prof. Wjst:
I am writing about your recent letter to the editor. We sent your concerns to authors of the studies you referenced and reviewed the replies we received as well as the studies themselves. I am sorry to say that your letter was not accepted for publication. We believe that limitations you raise were adequately acknowledged by the authors in the published papers and/or were consistent with reporting practices at the time of publication.
Thank you for the opportunity to consider your letter.
Sincerely,
Eric Rubin, MD, PhD
Editor in -Chief
So the New England Journal of Medicine has resolved my concerns about five hygiene hypothesis papers by consulting the authors. One is deceased. The rest are retired. All confirmed their work was fine, a somewhat predictable outcome.
The NEJM calls this research integrity. I call it a new normal: where the bar for correcting the scientific record is the posthumous approval of those who created it. The new normal – figures citing the wrong sources, null results missing from abstracts, undisclosed sample exclusions and a key figure that rests on an unpublished personal communication that has never been replicated. This is an interesting new benchmark for a journal of the NEJM's standing.
One for the files.
I am collecting material for an article questioning EBM (evidence based medicine) while coming across an interesting preprint by Zach Shahn “Trust me, I’m a doctor”.
Suppose that outcomes under usual care, e.g., collected from hospital health records, outperform the outcomes in both arms of a randomized experiment conducted in the same population. A textbook example concerning lung cancer patients comes from Hernan and Robins [2024], see also Sarvet and Stensrud [2025]. Then, Deaton and Cartwright's argument that one should trust their physician over a trial is validated. In this case, a next step is to find the criteria that physicians are using to make personalized decisions.
He continues to examine study settings in which a randomized trial is nested within an observational cohort, so that outcomes are observed under treatment, control, and usual care while I am following up here his reference to Sarveed & Stensrud Unfortunately the abstract of this paper is poor – it should have explained the two definitions of “harm” in personalized medicine. So I try it on my own.
Counterfactual harm – a patient is harmed if they received a treatment whose outcome is worse than what would have happened under the alternative – requires knowing unobservable potential outcomes / principal strata. The interventionist harm (the authors’ preference): a patient is harmed if their expected outcome under the assigned treatment is worse than under the alternative, conditional on their measured features which requires only experimentally identifiable quantities. The counterfactual approach is practically problematic because principal strata are metaphysical objects that can never be verified, require non-experimental data and partial identification. The interventionist approach is transparent, observable, and doesn’t coerce commitment to unverifiable metaphysics.
The paper does not explain how to do this in practice – I think this could be just a well-designed RCT with pre-specified effect modification analysis. The workflow would be; pre-register → stratified randomization → interaction-term analysis or causal forest → decision rule by argmax of expected outcome. You never need to ask “what would have happened to this patient under the other treatment” - you only ask “what does the evidence say about patients like this one.”
After dismantling USAID in January 2025, the Trump administration has been negotiating bilateral health agreements with over 30 countries, predominantly in Africa, under its “America First Global Health Strategy.” The deals tie what was previously humanitarian assistance to a bundle of strategic demands:
1. Personal health and genomic data
Ghana walked away from a $109 million deal after Washington demanded access to personal health data (Ärzteblatt, April 2026). In Zambia, the US demanded 10 years of access to national health and genomic data in exchange for only 5 years of funding, with no guarantee that Zambia would benefit from any vaccines or drugs developed from that data (IBTimes UK).
2. Mining concessions for US companies
A leaked State Department memo proposed explicitly using HIV aid for Zambia’s 1.3 million PEPFAR-dependent patients as leverage to extract access to copper, cobalt, lithium, and rare earth minerals (FPRI, March 2026). In the DRC, after demanding 20-year corporate tax exemptions, windfall tax waivers, and duty-free treatment for US imports, Washington secured a deal giving US firms right-of-first-offer on certain mining sites (Capital & Main, April 2026).
3. Recipient country co-financing
Zambia’s proposed deal required the country itself to contribute roughly $340 million in domestic health spending alongside the US offer of $1 billion over five years, sharply reducing the net benefit (Observer Research Foundation, March 2026).
4. Regulatory reforms favoring US investment
Several agreements include clauses requiring recipient governments to create favorable regulatory environments for US direct investment in mining and pharmaceuticals (Al Jazeera, April 2026).
So the strategic goal is to redirect African critical minerals - cobalt, copper, lithium, rare earths - into US supply chains and counter China’s dominance in African mining.
PEPFAR, long regarded as one of America’s most successful humanitarian programs (credited with saving over 26 million lives globally), is now being openly wielded as a negotiating tool. Zimbabwe, Zambia, and Ghana have rejected or walked out of talks; Kenya, Nigeria, Ethiopia, and over a dozen others have signed agreements. Malawi’s Kayelekera uranium mine restarted and now shipping to the US.
Critics, including former USAID officials, have called the approach “coercion dressed in the language of strategy.”
The 1972 Stockholm Declaration is considered a landmark in international environmental law, but it has not achieved its full potential to reverse ecological destruction.
Nice, that now also this paper finally appeared – it explains why also the Sabel and Larhammar 2025 Declaration will never work.
I recently came across the European Journal of Translational Myology publishing papers outside the scope of the journal and outside the expertise of the editorial board.
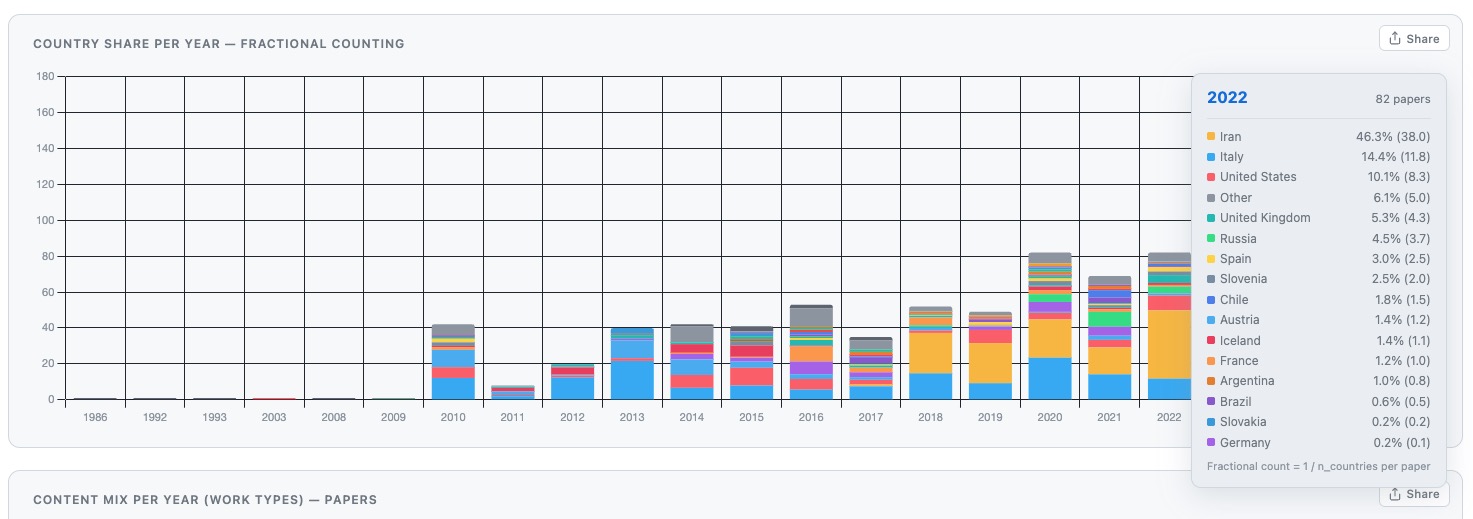
Editor-in-Chief Ugo Carraro (*1943, former University of Padua researcher) supported EJTM’s broadening from muscle physiology into general medicine, proposing a rename to “Myology, Mobility, Medicine”. The journal subsequently started to publish Iranian clinical papers across orthopedics, dentistry, psychiatry, COVID-19, and urology – not related to myology. In 2022, an Iranian author even published in EJTM a bibliometric study of Iranian output in EJTM itself – a self-referential feedback loop that normalizes the journal as a legitimate Iranian venue inviting further submissions.
The Cegolon bridge
Luca Cegolon (University of Trieste) is the structural intermediary between Baqiyatallah University of Medical Sciences (BMSU) and Italian academia. He holds at least six joint publications with Einollahi and Javanbakht spanning COVID-19, plasma exchange, ozone therapy, and kidney injury – all on Iranian data. Cegolon completed his PhD at Padua University Medical School, the same institution as Carraro. The Tehran-Trieste-Padua route therefore carries manuscripts from a sanctioned IRGC institution to a Pavia open-access publisher with no regulatory friction.
Javanbakht as serial off-topic submitter
Javanbakht’s EJTM papers cover kidney transplantation pharmacology (Suprotac tacrolimus), male fertility / varicocelectomy, and wrist tendon transfer surgery – none touching myology. The pattern is deliberate: EJTM is Scopus-indexed, open-access and has demonstrated tolerance for off-topic Iranian clinical submissions. The Suprotac APC was almost certainly paid by NanoAlvand Company, the product’s manufacturer, paying a trivially small marketing cost for a PubMed-citable Phase IV label.
The sanctions geography
From March 2013, OFAC regulations prohibited US-owned journals from handling manuscripts authored by Iranian government employees. Elsevier instructed its US editors to reject such manuscripts outright. OFAC sanctions also generated misunderstanding among editors in other countries, who rejected Iranian manuscripts for political rather than scientific reasons, further narrowing the accessible publishing landscape.
The primary exchange is probably not financial but metric. For Cegolon, co-authorship with a high-volume Iranian clinical group accelerates publication output at a career stage where Italian Abilitazione Scientifica Nazionale metrics directly determine promotion. For BMSU and NanoAlvand, the European co-author provides editorial access, institutional legitimacy, and a sanctions-circumventing pathway to Scopus. The APC is the transaction cost; mutual bibliometric benefit is the structural incentive - legal, common, and largely misaligned with quality control.
Reactions
15/6/26 I received an email from Ugo Carraro that basically confirms that <EJTM3 has opened up since 2018 to publish any “Medicine” work>. Interestingly he adds that all
Ejtm papers end with the Disclaimer: All statements expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, nor those of the publisher, editors, or reviewers. Any product reviewed in this article or claims made by its manufacturer are not guaranteed or endorsed by the publisher.
So he distances from the content – a strange move. Sure, as a liability device, it is a standard, boilerplate non-endorsement clause found across many journals. Under ICMJE and COPE norms, editors retain responsibility for what they accept, including registration requirements, scope fit, and conflict-of-interest handling. A publisher cannot contract out of that responsibility after the fact via a footer. The disclaimer does not address why a prospectively-unregistered, manufacturer-funded bioequivalence study was accepted in a myology journal. The authors responded with some AI generated appeasement while the publisher response is still missing.