If paracetamol use in pregnancy may cause later autism spectrum disorder has received public interest recently.
Robert J Lifton wrote in “Losing reality”
Trump is different. His solipsism is sui generis. He is psychologically remarkable in his capacity to manufacture and continuously assert falsehood in the apparent absence of psychosis.
Not unexpected the advice was rejected by basically all medical professionals. Commentaries are raging in Nature, BMJ , The Lancet, JAMA and even the WHO.
The World Health Organization (WHO) emphasizes that there is currently no conclusive scientific evidence confirming a possible link between autism and use of acetaminophen (also known as paracetamol) during pregnancy.
Most recently six surgeons general warned even about RFK jr.
Yet Kennedy continues to ignore science and the public’s wishes. Most recently, HHS proposed new warning labels on products containing acetaminophen (Tylenol), citing a supposed link between prenatal use and autism. This move has been widely condemned by the scientific and medical communities, who have pointed out that the available research is inconclusive and insufficient to justify such a warning. In an extraordinary and unprecedented response, the American Academy ofPediatrics, the American College of Obstetricians and Gynecologists and other leading health organizations issued public guidance urging physicians and patients to disregard HHS’s recommendation. Instead of helping pregnant women make informed decisions during a critical period in their lives, Kennedy’s decisions risk causing confusion, fear and harm. Rather than combating the rapid spread of health misinformation with facts and clarity, Kennedy is amplifying it. The consequences aren’t abstract. They are measured in lives lost, disease outbreaks and an erosion of public trust that will take years to rebuild.
So let’s have a look at the main paper that caused this storm. Who is writing what and why?
The first author DP is a MD with a publication record at Scholar showing an IF of 23 over a period of 16 years. He proudly shares at Linkedin that his research is even discussed at FOX News … The second author BR is a German MD, known for previous dubious claims that I have discussed at Deutsche Ärzteblatt. The third author AZB has a BS in Industrial Engineering and Epidemiology and first authored just 4 papers in the last 12 years including a “consensus statement” about paracetamol that was heavenly criticized (ref, ref). The last author Andrea Baccarelli s an Italian MD/PhD. The Times described him
Scientist behind Trump’ s Tylenol claims was paid $150K to give evidence against drug maker. The Harvard academic Andrea Baccarelli gave an ‘unreliable’ testimony on the links between autism and paracetamol, and produced research that raises ‘serious concerns about bias’.
The court decision did not leave any doubt about his earlier testimony
… Dr. Baccarelli also disregards relevant reviews of epidemiological studies conducted by medical and governmental associations. He does not address the FDA’s repeated conclusion that the epidemiological evidence does not support his opinions, other than to note his disagreement with that conclusion. Nor does he grapple with the contrary conclusions of the American College of Obstetricians and Gynecologists, the Society of Obstetricians and Gynaecologists of Canada, or the European Network of Teratology Information Services. This “rejection of a conclusion that could not be more relevant to his opinions is alarming.” In sum, Dr. Baccarelli failed to sufficiently explain the appropriateness of conducting a single Bradford Hill analysis for NDDs which included ASD and ADHD, selectively analyzed the consistency of the literature and the issue of genetic confounding, repeatedly pressed conclusions that study authors were not willing to make, and disregarded studies that do not support his opinion due to limitations that he did not view as disqualifying in studies that did support his opinion. Together, these deficiencies demonstrate that his opinion does not “reflect[] a reliable application of the principles and methods to the facts of the case.”
So the “who” question could be easily answered. The two authors with the lowest qualification (AB and DP) selected the studies and assigned the scores while there was no expert in pharmacoepidemiology or any author involved with more than casual experience in meta-analysis or autism research. The answer to the “why” question is also be obvious – Baccharelli would have to pay back his $150K if he would publish now the opposite.
We can therefore move on to the more important “what” is in this “rigorous review”.
Unfortunately I am already stuck at the abstract. It says that 27 positive, 9 null and 4 negative studies were included (in total 40) but continues with 46 studies. The included chart has even two more internal contradictions that can be found immediately. Can you find them? Riddle solution is in the next table.
I 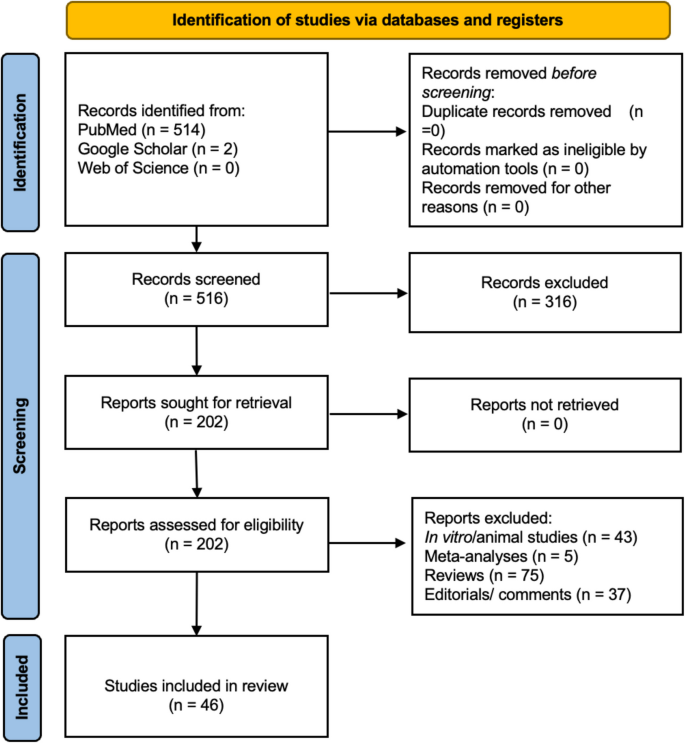
Reading the result text and the tables is even more confusing. So I am reconstructing here the study numbers.

I can only speculate what happened here – some errors (eg 514 vs 518) must have already been present in the initial version while most errors have been introduced during the revision as a reviewer asked for the grading tables. Some studies were missed during grading and then errors were back propagated even to the abstract.
Studies have also been wrongly reported. Already the first study in table 1 has a wrong CI (it is of course 1.05-1.10). The second study gives a wrong sample size (the 31,156 are discordant on exposure, not on outcome!) although I am not going to check this further.

What about the confounder reported? Their effect is not equal according to previous research.
For neurodevelopmental disorders especially, they are highly heritable, and genetics comprises a substantial proportion of their cause. So studies that don’t take into account genetics may come to different conclusions than studies that do take into account genetics.
But how did the authors define the bias classes? Just by eyeballing? Or any SOP? Why has the most important confounder even be omitted from the analysis?
Studies were rated as higher risk of bias (score of 3 or 4) if they lacked adjustment for key confounders, such as maternal age, chronic illness, socioeconomic status, smoking, alcohol use, or clinical indications for acetaminophen use (e.g., fever or infection).
One more thing: The authors describe basically no bias in autism outcome which is in contrast to more recent research that show a mixture of different age-dependent polygenic traits. Unfortunately age of diagnosis was never considered by the authors.
If exposure and and outcome in ASD studies are so heterogenous, we can believe in one or the other study. But there the overall conclusion is not supported that “immediate steps should be taken to advice pregnant women to limit acetaminophen consumption”. Also the primary Environmental Health reviewer has noticed this framing. The authors politely replied that
We acknowledge the need for a balanced presentation and recognize that our initial framing may have appeared to favor positive results.
but simply kept their narrative construction to shape the political discourse at the cost of scientific integrity.
Postscript 1
Bonus point for the 4 authors, the 3 assistants in the acknowledgment, the 2 reviewer and the 1 editor for leaving an internal bold marked comment in the PDF on page 12.
Postscript 2
My Pubpeer review has been submitted to Philippe Grandjean (editor of Envir Health) on 9Oct25 with no response. Another email went to ethics.reporting@springernature.com on 12Oct25 with an automatic reply
As a member of the Committee on Publication Ethics (COPE) we take all concerns about the research integrity and publication ethics of our content seriously and will investigate. Details of our investigations are confidential and will not be shared. However, we will notify you of the outcome of our investigation once an editorial resolution has been reached.
Postscript 3
Baccharelli talked in advance of this paper to RFK jr. It seems that Kennedy is not convinced and will provide “the proof” at short notice.