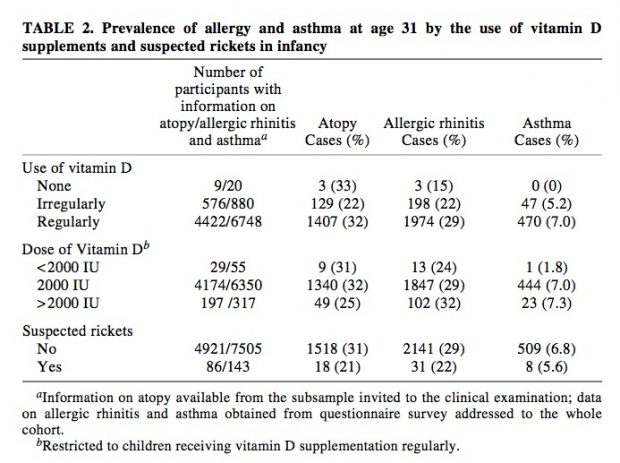
A clinical study in 2015 already showed, how to recognize vitamin D responders using a preselected gene set based on VDR chip seq data.
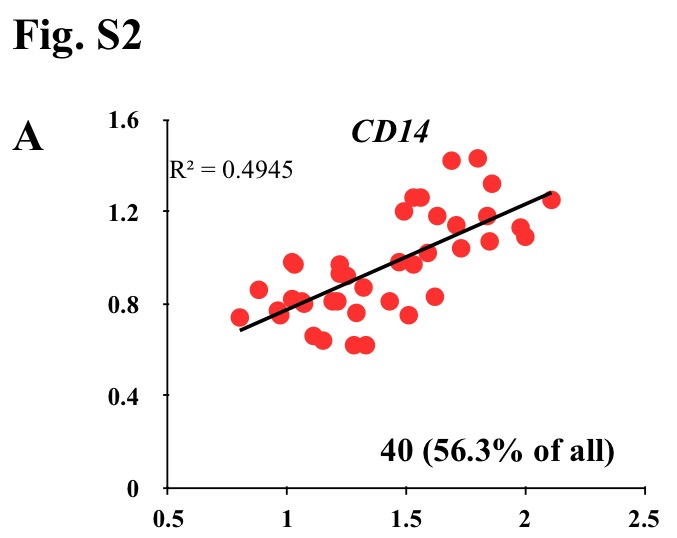
Vitamin D3 is a pleiotropic signaling molecule that has via activation of the transcription factor vitamin D receptor (VDR) a direct effect on the expression of more than 100 genes. The aim of this study was to find transcriptomic and clinical biomarkers that are most suited to identify vitamin D3 responders within 71 pre-diabetic subjects during a 5-month intervention study (VitDmet). In hematopoietic cells, the genes ASAP2, CAMP, CD14, CD97, DUSP10, G0S2, IL8, LRRC8A, NINJ1, NRIP1, SLC37A2 and THBD are known as primary vitamin D targets […] only 39-44 (55-62%) of the study subjects showed a highly significant response to vitamin D3, i.e., we considered them as "responders" … genes were expressed but in a wide range that differed up to 327-fold between the most prominently (CD14) and the lowest expressed candidate (CAMP)
y-axis end/start CD15 serum, x-axis end/start 25-OH-D3
In new editorial, the same authors argue that the vitamin D response index is an epigenetic property of an individual that may not change at all. Indeed, changes in the epigenome, such as methylation of genomic DNA is an essential prerequisite for initiating gene transcription. The concept of an individual vitamin D response therefore has a lot of merits and is able to resolve a long controversy which serum vitamin D levels are sufficient.
CD14 is a particular interesting gene. As we have learned in allergy research, however, methylation status is not stable over time, it increases slightly over the first decade, possibly as vitamin D sensitivity decreases??
The average increase in CD14 methylation from 2 to 10 yr (n = 153) was 1.3% (from 5.5% to 6.8%, p = 0.001)
This difference isn’t really huge while also the time spent outdoors seem to be relevant. CD 14 methylation may even influence SNP association results
rs2569191, rs5744455, and rs2569190 were associated with sCD14 levels at birth and 2 years, but only rs5744455 was associated with sCD14 levels at 10 years. CD14 methylation increased significantly from age 2 to 10 years.
So CD14 methylation looks like an interesting indicator and may even have biological relevance itself as CD14+ monocytes can differentiate into a host of different cells.
CC-BY-NC Science Surf , accessed 28.07.2026