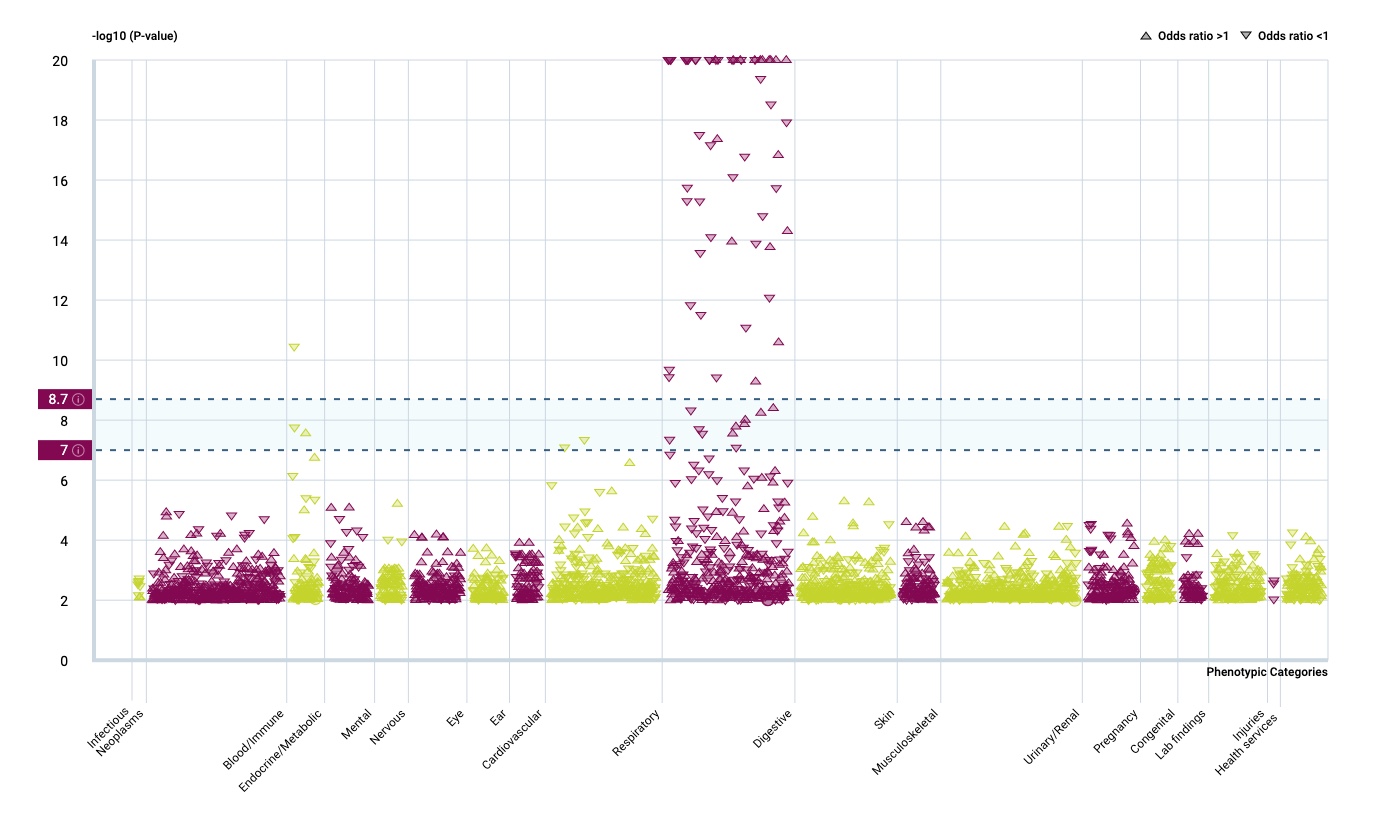
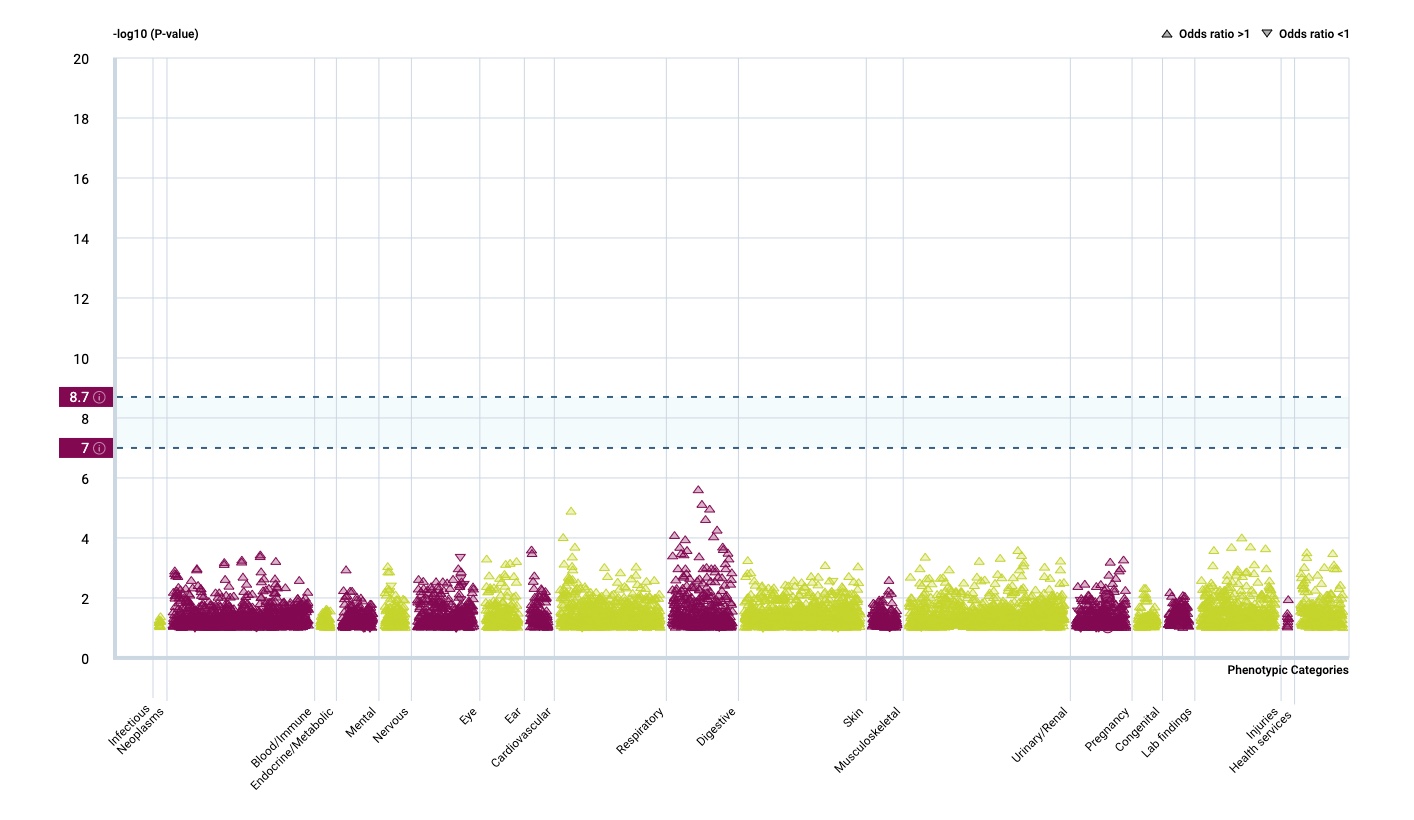
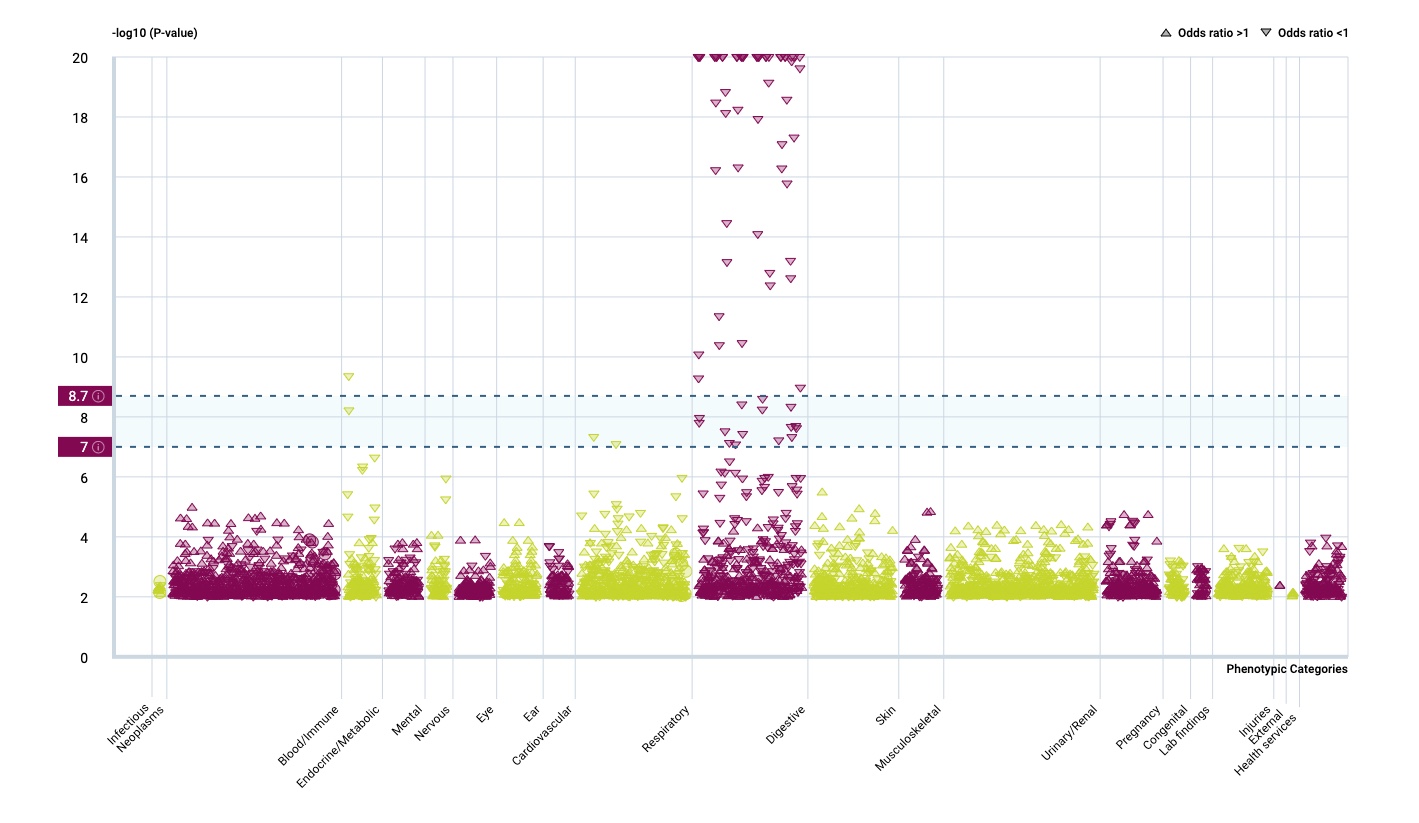
It seems that I missed an interesting 2017 paper that looked for disease-associated SNPs in canonical DR3 motifs. Only 7 out of 211 traits showed significant hits, one of these was self-reported allergy. When annotating these SNPs, there are only two genes: LINC00299 and TLR1
hg38 position
rs10174949 2:8302018 LINC00299
rs10178845 2:8303773 LINC00299
rs5743566 4:38804221 TLR1
rs2101521 4:38809830 TLR1
rs5743565 4:38804262 TLR1
rs45588337 4:38805607 TLR1
rs55830619 4:38805643 TLR1
So are TLR1 & LINC00299 variant carriers more susceptible to vitamin D induced allergy?
LINC00299 (Long Intergenic Non-Protein Coding RNA 299) is a RNA Gene of largely unknown function, associated so far with allergy only on a genetic level in Framingham, href=”https://pubmed.ncbi.nlm.nih.gov/23817569/”>23andme and other studies. We don’t know so much here, the function of the long non coding RNAs
depends on subcellular localization. Depending on their niche, they specifically interact with DNA, RNA, and proteins and modify chromatin function, regulate transcription at various stages, forms nuclear condensation bodies and nucleolar organization. lncRNAs may also change the stability and translation of cytoplasmic mRNAs and hamper signaling pathways. Thus, lncRNAs affect the physio-pathological states and lead to the development of various disorders, immune responses, and cancer.
The TLR1 genetic association is found by many genetic studies, while the clinical association is probably more by an infectious origin. TLR1 is a pattern recognition receptor with a specificity for gram-positive bacteria and also included in my forthcoming exome paper as a protective factor for asthma/allergy. And we are also close to my earlier review of vitamin D, the microbiome and allergy…
Does any co-infection response during first vitamin D exposure influence allergic sensitisation? There are indeed some hints of an short-lived effect of lung group 2 innate lymphoid cells (ILC2s)
Laboratory mice cohoused for 2 weeks had impaired ILC2 responses and reduced lung eosinophilia to intranasal allergens, whereas these responses were restored in mice cohoused for ≥2 months. … These findings suggest that ILC2s respond dynamically to environmental cues and that microbial exposures do not control long-term desensitization of innate type 2 responses to allergens.